-
Urban Resilience: What Is It and How Can We Promote It?
›A new study on the intersection of violence and economic development in cities breaks new ground by examining how communities respond to and cope with extant violence, rather than focusing on the root causes of violence in a given area. Authors Diane Davis, Harvard professor of urbanism and development, and John Tirman, executive director of MIT’s Center for International Studies, spoke at length about the origins, methodology, and findings of the report, Urban Resilience in Situations of Chronic Conflict, at the Wilson Center on July 12. The report was supported by USAID’s Office of Conflict Management and Mitigation.
“We made the decision that we weren’t going to produce yet another research project or study on the root causes of violence, because there is a lot of incredibly good work on that [already],” said Davis. “We wanted to take a totally different angle…to try to think about taking a more pragmatic approach that builds on how everyday people, who live with violence, respond.”
To do this, Davis and Tirman focused their research on seven cities around the world with histories of chronic violence, creating a case study for each and then comparing results. (An eighth city, Karachi, was jettisoned because it was deemed too unsafe for research.) The comparative process allowed Davis and Tirman to develop a basic theoretical framework for how different factors increase or decrease a community’s resilience to violence.
Defining Resilience
The term “resilience” lies at the heart of the new study. “The idea of ‘bouncing back,’ or returning to normalcy, is [generally] the measurement standard for looking at resilience,” Davis said.
However, she was quick to point out the problems with such a simplistic definition. “[In] cities of the developing world…things are in flux. So it’s really hard to know what a ‘bouncing back’ is if things are constantly changing.” “Also,” she added, “in many of the environments we were looking at, violence is a consequence of the way things were under normal conditions. So you don’t necessarily want to bounce back to those conditions that were producing the violence in the first place.”
“Also,” she added, “in many of the environments we were looking at, violence is a consequence of the way things were under normal conditions. So you don’t necessarily want to bounce back to those conditions that were producing the violence in the first place.”
Davis and Tirman sidestepped these problems by letting their research define successful resilience, rather than trying to fit their results to a prefabricated definition of the word. In doing so, they were able to identify several important commonalities in the cities and communities that displayed the most positive resilience to violence.
“Our findings suggest that resilience appears at the interface of civilian and state action,” Davis writes in the report. She underscored the significance of civilians as facilitators in both developing and implementing better security policies: “People who live in violence know more than academics or policymakers about what they can and can’t do to deal with the problem of violence,” she said.
Focus on Community
Davis and Tirman pointed out that the most successfully resilient cities they studied – Mexico City, Managua, and especially Medellín – seemed to have a number of civilian/state relationships defined “from below,” rather than the more problematic “top down” approach. This means that civilians and communities were participating on their own terms, collaborating with city planners and with law enforcement agencies to get their needs met rather than simply being what Davis called “yes men” to higher authorities.
Physical space – what Davis referred to as “the weight of the spatial” – also played a very significant role in Urban Resilience. She and Tirman made the conscious decision to incorporate physical planning and design into their research, eschewing the more typical sectoral approach to violence and security.
This methodological break from the existing literature was particularly useful in demonstrating that violence-plagued communities are often themselves the most important agents of resilience. “Citizens have to be able to make real decisions on their own,” Davis stressed in the Q&A; session that followed her and Tirman’s presentation. “[They] have to feel that ownership, that autonomy of the decisions in their neighborhood, even if they’re bad [decisions], because that’s what ties them to each other.”
“We think the starting point for generating resilience is really supporting and enabling communities to make dense horizontal relationships with others in their neighborhood, across sectors, that allow them to push back against perpetrators of violence.”
In other words, while the state can play a significant role in helping communities to mitigate violence, successful resilience ultimately requires the commitment and participation of the communities in question.
“The state might have a security program, it might have a planning program, but every decision has to be made with an understanding of what’s good for that particular neighborhood,” Davis said.
Places People Want to Protect
Davis was very succinct in offering recommendations based on the study. For policymakers and urban planners, she said resilience is formed by “a combination of good governance, security reform, and…inclusive urban planning.” Citing examples from Mexico City, Medellín, and elsewhere, Davis pointed to planning policies like mixed land use, greater pedestrian accessibility, and more parks and public spaces as ways that authorities could engender the kind of community pride so crucial to the development of positive urban resilience.
“[Focus on] generating vibrant public areas where people feel invested in protecting [them] and making them better,” she advised.
While many scholars have tended to look either at the state or local communities in isolation when considering violence and resilience, Davis argued that reducing violence was “a shared objective.” She thus stressed the importance of “co-production of security,” reiterating the overall notion that state and community actors need to work side-by-side in a form of what Davis and Tirman called “cooperative autonomy.”
In addition to Urban Resilience in Situations of Chronic Violence, Davis also authored the supplementary Toolkit for Urban Resilience in Situations of Chronic Violence. Both documents can be found on the MIT’s website. Davis and Tirman hope to add the seven individual case studies to the site soon.
Event Resources:Photo Credit: “Bogota at night,” courtesy of flickr user WanderingtheWorld (Christopher Schoenbohm); charts courtesy of Davis and Tirman. -
‘Motherland Afghanistan’ Shows Maternal Mortality Not Just A Health Issue
›Afghanistan has one of the highest rates of maternal mortality in the world: 327 out of every 100,000 women who give birth die during childbirth. Despite some recent improvements, political, social, cultural, and economic factors present enormous challenges. Last month, the Center for Population and Development Activities hosted an online viewing and dialogue discussion of the PBS Independent Lens film Motherland Afghanistan, which follows Afghan-American filmmaker Sedika Mojadidi and her father, Dr. Qudrat Mojadid, as they return to their home country and visit the Laura Bush Maternity Ward in Kabul. The conditions they find are devastating and underscore not only the need for greater commitment to reproductive health services, but also the advancement of women’s and girl’s access to education, security, and political participation.
-
Nancy Lindborg, The Huffington Post
Chronic Crisis in the Sahel Calls for a New Approach
›July 10, 2012 // By Wilson Center StaffThe original version of this article, by Nancy Lindborg, appeared on The Huffington Post.
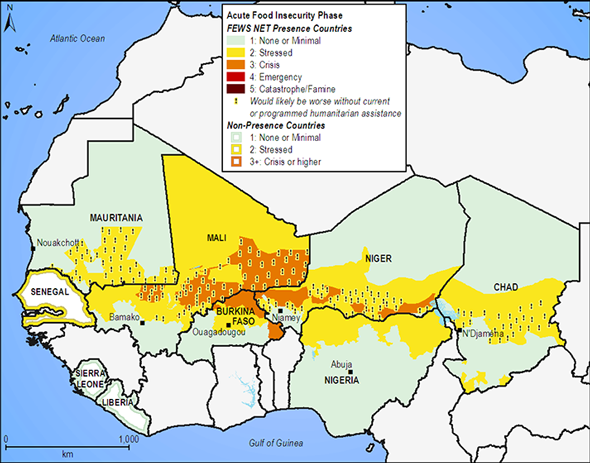
It is the lean season in the Sahel, a spine of arid and dry lands that runs from Senegal to Chad in western Africa, and once again we are seeing the devastating images of children gaunt with hunger. This is a region that faces high childhood malnutrition and underdevelopment even under the best of circumstances so one poor harvest can push millions of the most vulnerable into severe risk. In the aftermath of poor rains, and with food prices stubbornly stuck on high since the food crisis of 2008, some 18.7 million people across eight affected countries in the Sahel are at risk of food insecurity this year alone. At least eight million people are already in need of emergency assistance.
At USAID, we are determined to get ahead of these kinds of chronic crises. We know that millions of Africans living in the dry lands of the Horn and Sahel regions need new solutions. Last year, the worst drought in 60 years ravaged the Horn of Africa, driving 13.3 million people into crisis. And this summer, families in the Sahel are feeling the peril of depleting food supplies, high food prices, and rising malnutrition.
We can’t prevent what appears to be increasing cycles of drought, but we can and are working to create better solutions and build greater resilience among the most vulnerable.
Every crisis is complex, and the Sahel is no exception. A regional drought has been overlaid with instability stemming from the coup in Mali and conflict in the northern part of that country where armed militant groups have forced the suspension of critical relief operations. More than 184,000 refugees have fled to communities in neighboring countries that are already deeply stressed from drought. Though still functioning, local and regional markets have been disrupted, driving food prices even higher. And as of mid-June, swarms of locusts from southern Algeria and Libya had arrived in northern Mali and Niger; now expected to move southward, these infestations could result in crop destruction exacerbating an already worsening situation.
Continue reading on The Huffington Post.
Image Credit: West African medium-term food security outlook, courtesy of the Famine Early Warning Systems Network.
Nancy Lindborg is the assistant administrator of the Bureau for Democracy, Conflict, and Humanitarian Assistance at the U.S. Agency for International Development. -
USAID Turns to Crowdsourcing to Map Loan Data
›
The original version of this article, by Aaron Lovell, appeared on the Wilson Center’s Science and Technology Innovation Program Commons Lab blog.
On June 28, officials from USAID met at the Wilson Center to discuss a recent experiment in using crowdsourcing to help clean up and map data on development loans. The agency had 117,000 records on private loans made possible by their Development Credit Authority, which theoretically could be mapped and made available to the public. The problem? Location data for the loans was not standard and was difficult to parse. USAID decided to turn to “the crowd” and recruit interested volunteers from the Standby Task Force and GISCorps – two online volunteer communities – to help clean the data, making it available for additional analysis.
Shadrock Roberts, Stephanie Grosser, and D. Ben Swartley – all with USAID – discussed the results of the project. They were able to clean up the information at virtually no cost to the government, noting that they hope it will be an example for further collaboration between government and engaged volunteers.
“Our hope is that the case study will provide others in government with information and guidance to move forward with their own crowdsourcing projects. Whether the intent is opening data, increased engagement, or improved services, agencies must embrace new technologies that can bring citizens closer to their government,” the officials wrote in a recently released case study focused on the exercise. While the exercise resulted in high-quality output, Roberts et al. did provide advice for other agencies considering similar work. Grosser stressed the need to “crawl, walk, [then] run” – that is, start small with a few hundred records and then expand on that, as the system is refined.
But USAID sees crowdsourcing becoming a key part of improving government data. “We need to be working as hard to release relevant data we already have as we are to create it,” Roberts concluded, when discussing how the experience could apply more generally. “The crowd is willing to do research, data mining, and data cleanup.”
Sources: USAID. -
Book Review: ‘World Population Policies’ Offers Sweeping Overview of a Complex Field
›July 2, 2012 // By Elizabeth Leahy MadsenWith much attention in the international family planning community directed to the impending anniversary of the 1994 International Conference on Population and Development and the closing date of the Millennium Development Goals, the fact that 2012 is the 60th anniversary of two other milestones in population programming may have escaped notice. In 1952, the International Planned Parenthood Federation was created, and India became the first country to formulate a national policy to reduce population growth.
These and many other landmarks are highlighted in World Population Policies: Their Origin, Evolution and Impact, a new book by demographer John May that reviews several decades of policies, advocacy, and program interventions addressing the full range of diverse demographic trends seen globally.May, who spent more than two decades working on population issues at the World Bank and other international institutions before recently assuming a fellowship at the Center for Global Development, is well-positioned to provide such an ambitious overview. Although the breadth of material included in the book means that some topics receive less coverage than a specialist might wish, it serves as a sound introduction to this diverse field, and offers some particularly interesting case studies.
The book’s main chapters begin with a summary of current population trends, including a comprehensive array of figures and statistics about population size, distribution, and projections. Some important concepts, such as the demographic transition and dividend, are perhaps covered too quickly, and in such cases the book would have benefited from more than a handful of figures, charts, and graphs. May classifies regions and countries as demographic “hotspots,” where the number of people outstrips available resources, and “coldspots,” which have too few residents. He makes an ambitious suggestion that high-density countries facing resource challenges, such as Bangladesh, should consider promoting rapid fertility decline below replacement level to stop population growth, then reverse course and increase to a rate that promotes a stable population – but such a reversal from low fertility is a feat that has stymied several countries in Europe and East Asia.
Evolution of the “Population Movement”
In addition to summarizing the ways that demographic issues have been framed in the past several decades, May briefly describes the long-running debate between demographers and economists about the ways in which population is theorized to affect economic development.
Three points in this chapter were particularly striking: First, the concept of family planning as a human right dates from well before the 1994 International Conference on Population and Development. In 1968, the Tehran International Conference on Human Rights defined the ability to choose family size and spacing as a fundamental right; still, some programs, such as India’s under the Emergency-era government of the late 1970s, adopted coercive practices. Second, population policies are not limited to official initiatives targeting fertility, mortality, and migration, but also encompass implicit or “passive” policy measures that arise without advance planning or that have an unintended effect on demographic trends. Related to this, May suggests that “contextual variables” such as education, health, gender, culture, and religion can have a greater impact on population policies’ effectiveness and demographic outcomes than government structures or funding.
Although population policies are most often designed at the national level, May’s discussion of the “population movement” highlights the influence of international networks and donors on such policies. By the late 1960s, the U.S. Agency for International Development had begun funding family planning programs overseas, and the United Nations Population Fund (UNFPA) was active. Although the United States has become less dominant over time, population programming remains a Northern-driven movement.
Beginning with a meeting in Belgrade in 1965, a series of international population conferences successfully raised the prominence of population issues on the global development agenda and built consensus around international goals, while also becoming increasingly political.
May’s cautions about such conferences are timely given this month’s London Family Planning Summit: “Consensus-building through international conferences and their preparatory meetings is often inefficient as a process, whereas such events could be used to promote learning among policymakers and experts…The gap between the conferences’ resolutions and the actual policies implemented at country level is important to remember” (110).
Growth and Aging Distinguish the Demographic Divide
In his chapter focusing on the developing world, May notes that population policies have become broader in the nearly 20 years since the Cairo conference, incorporating a reproductive rights framework while also addressing new issues such as the environment, HIV/AIDS, and poverty. But under this more holistic approach, national policies are susceptible to becoming overly diffuse, with an ambitious agenda not matched by concrete action plans.
The challenges expand to policy implementation as well. Kenya is profiled as emblematic of the difficulties facing population programs in fast-growing sub-Saharan Africa, particularly political disinterest, mismanagement, opposition from some religious groups, and commodity shortages. But when implemented well, such policies can be very successful. The book offers a thorough summary of research findings on the common features of effective family planning programs (such as leadership, monitoring performance data, and opening access to contraceptive methods at lower levels of the health system), as well as their demographic impact. Several country examples are cited to show that family planning programs reduce lifetime fertility rates by 0.5 to 1.5 children per woman, while also benefiting individual and social health, income, and well-being.
While population policies have been often effective at shaping demographic trends in high-fertility settings, even in changing cultural norms about family size, May notes that their impact has been notably weaker in reversing the trajectory of declining fertility in developed countries. While countries such as France have maintained a fertility rate close to, albeit still below, replacement level thanks to generous paid parental leave, housing initiatives and public child care facilities, policies that try to boost low fertility through financial compensation have been particularly ineffective.
Developed countries are less likely to have formal population policies and tend to address demographic issues through incentives and disincentives implemented by multiple agencies. Aging and immigration are receiving greater attention in such countries, along with low fertility rates. Population aging raises policy concerns that are both economic and social, and May focuses largely on the benefit of reducing incentives for early retirement. He notes that thanks to improvements in health and life expectancy, “today’s 65-year-old persons are young compared to their counterparts” of previous generations (180). Despite their economic soundness, government efforts to raise retirement ages are widely unpopular, and France’s newly elected president has promised to cut the retirement age from 62 to 60 for some workers.
What Comes Next
Some observations are intriguing and could have been further detailed. For example, May notes a recent “fragmentation” of organizations working on population issues, and suggests that “too many institutions and NGOs appear to support their own limited mandates as they also struggle for resources that are less abundant” (5). Decentralization and integration within health systems is a growing trend that could have been discussed in more detail, along with the legacy of pronatalist laws and attitudes by colonial powers in Africa, the effect of recent European efforts to tighten immigration policies, and the achievements of forums designed for collaboration on population policy issues (for example, the United Nations Commission on Population and Development or the Reproductive Health Supplies Coalition).
Looking towards the future, May foresees continued integration of demography with related development issues, such as poverty reduction and equitable growth, gender and youth perspectives, environmental issues, and conflict prevention. He notes a few challenges, including sub-Saharan Africa’s lag in fertility decline and the overall ineffectiveness of policies aimed at addressing the pressures of urbanization on infrastructure and resources.
In high-fertility settings, May recommends that instead of framing reproductive health writ large, policies should more specifically target family planning and women’s empowerment, including education and income-generation opportunities as well as legal rights. Bangladesh is presented as a model for other countries, as a setting where cultural change and economic development laid the groundwork for successful family planning outreach efforts. Most of all, May entreats government leaders to maintain a policy focus on population issues, regardless of where they stand in the demographic divide.
Elizabeth Leahy Madsen is a consultant on political demography for the Wilson Center’s Environmental Change and Security Program and senior technical advisor at Futures Group.
Photo Credit: “Crowded Shopping District,” courtesy of flickr user EnvironmentBlog. -
Pop at Rio+20: Reproductive Rights Missing From Outcome Document – Assessing the Disappointment
›June 22, 2012 // By Sandeep BathalaAs heads of state get ready to sign on to the outcome document here in Rio, all eyes are on next steps – especially for the reproductive health and integrated development communities, which have seen their hopes of mainstreaming their issues with the sustainable development agenda dashed.
The final outcome document can be found here. USA Today reports that opposition from a group of countries in the 11th hour stripped the text of critical reproductive rights language:An initial draft of this conference’s outcome document stated, “We are committed to ensure the equal access of women and girls to education, basic services, economic opportunities, and health care services, including addressing women’s sexual and reproductive health and their reproductive rights.”
Absent entirely is any explicit connection between reproductive rights, population dynamics, and sustainable development.
In the final draft, the stronger wording “We are committed to ensure the equal access” was switched to the weaker “We are committed to promote the equal access.” The reference to reproductive rights was deleted altogether, after opposition from the G-77, a negotiating bloc of developing countries at the United Nations, and the Holy See.
But others, as we have heard repeatedly throughout the conference, insist that gender issues and reproductive rights have a strong and vital connection to sustainable development. Yesterday, USAID, the Aspen Institute, and the Center for Environment and Population held a discussion in the U.S. tent on this very issue, titled “Making Population Matter: The Demographic Dividend and Sustainable Development.”
As Vicky Markham of the Center for Environment and Population reports on RH Reality Check, the side-event aimed to demonstrate the effects of population dynamics, both positive and negative:We have the largest youth demographic ever in the history of the world, and most developing nations have a “youth bulge.” This can be seen as a challenge, or opportunity, particularly if the focus is on providing development programs for child survival, family planning, reproductive health, and education. The importance of women’s empowerment was also central. But it’s not a given; it’s an opportunity only if we pay attention to these issues to increase the benefits of the “demographic dividend.”
The demographic dividend, as described by USAID Deputy Administrator and panelist Donald Steinberg in blog post earlier this week, “is an opportunity that arises when a country transitions from high to low rates of fertility and child and infant mortality.” But it’s not just about ensuring access to family planning and reproductive health; youth-focused economic and education policies are also needed: “Maximizing the dividend requires social and economic policies that reinforce inclusion, equity, and opportunity across the entire population,” he writes. USAID is making a point of creating youth-focused policies for this reason, he said in Rio.
Carmen Barroso, regional director of the International Planned Parenthood Federation’s Western Hemisphere Region, pointed out that Latin American countries could not take advantage of the demographic dividend before recent societal changes occurred, including decreased fertility, increased urbanization (which leads to smaller families), and greater schooling and employment of women.
Seventy percent of world population growth is likely to be generated by Africa this century, said Eliya Msiyaphazi Zulu, executive director of the African Institute for Development Policy – and it is the only continent projected to continue to grow in the next century, he said. He called for redefining growth as more than GDP as that measure does not consider environmental degradation and its costs: “We must have other means to measure development.”
As heads of state and negotiators consider their positions at this conference – which many were hoping would make a much stronger statement – they might do well to ponder today’s comments from Secretary of State Hillary Clinton:While I am very pleased that this year’s outcome document endorses sexual and reproductive health and universal access to family planning, to reach our goals in sustainable development we also have to ensure women’s reproductive rights. Women must be empowered to make decisions about whether and when to have children. And the United States will continue to work to ensure that those rights are respected in international agreements.
Sources: RH Reality Check, UN, U.S. Department of State, USA Today, USAID.
Now none of this is an abstract discussion. There is just too much at stake, too much still to be done. And many of you visited the U.S. Center here in Rio and saw practical solutions related to some of the work I’ve discussed and other goals we hold in common. We believe solutions require action by all of us. Governments, yes; let’s do our part. Let’s do more than our part.
Photo Credit: YouthPolicy.org. -
Pop at Rio+20: Text Finalized, Population-Sustainable Development Links Left Out?
›June 21, 2012 // By Sandeep BathalaWhile I was visiting with youth peer educators yesterday with the Brazilian Society for Family Welfare in the Cachoeirinha favela (see Vicky Markam’s post for details – we were on the same trip), UN member states reached consensus in the Rio+20 negotiations. But, according to reports, although the outcome document includes some mention of reproductive health, gender equality, and women’s empowerment, it fails to explicitly recognize the link between reproductive rights and sustainable development.
Many women’s rights and health observers have, from the start, encouraged this link.
Karen Newman, speaking to ECSP in April during the Planet Under Pressure conference – a precursor to Rio – said she hoped this week would offer an opportunity to look at “sustainable development in the round” and “re-identify family planning as a core development priority,” given its human rights and health implications and relationship to population growth.
Jenny Shipley (Former Prime Minister of New Zealand) wrote just yesterday on CNN that “we are at a moment in history where we still have time to make a difference. It is essential that the global discussion in Rio not be blind to the potential solutions that access to voluntary family planning could offer to many of the world’s problems.”
“We can no longer afford this outrageous oversight, driven by old-fashioned tradition, discrimination, and pure ignorance,” said Gro Harlem Brundtland (Former Prime Minister of Norway and Former Head of the World Health Organization) at a side event on Monday. “Now is the time to agree to unleash the largest untapped potential for sustainable development and stop all discrimination against women and girls.”
But now that preliminary agreement on the outcome text has been reached, reports have filed in that the connection many were hoping for is absent. Zonibel Woods, blogging on RH Reality Check, wrote:From the start of the negotiations, gender equality and women’s human rights, including reproductive rights, have continuously been challenged by a few governments, claiming that [these] had “nothing to do with sustainable development.”
The lack of consensus among the wider international community may also undercut efforts to highlight reproductive rights in the post-2015 Millennium Development Goals/Sustainable Development Goals framework and as governments ready for the follow-on to the International Conference on Population and Development in 2014. A concrete link to “sustainable development,” whatever form that takes, would help ensure that reproductive health is not side-lined.
This debate continued until the last few hours of the negotiations. In the end, the text includes a re-affirmation of both the Cairo and Beijing agreements, but it falls short by failing to recognize that reproductive rights are also critical to the achievement of sustainable development. If a woman cannot decide if and when to have children and if she is not provided with the reproductive health care that is her human right, it is challenging to contribute to sustainable solutions for the planet.
Immediately following the adoption of the text, women gathered and protested at Rio Centro, the main venue for the conference, and advocacy continues.
Heads of state will in all likelihood sign on to the outcome document by tomorrow (it could technically still be changed, but that appears unlikely). I will keep you posted on the final outcome and will be taking notes at a side-event this afternoon by USAID, the Aspen Institute, and Center for Environment and Population on the demographic dividend and sustainable development, which promises to be spirited given today’s news. You can tune in live to the webcast of that event at 2:30 EST on Ustream.
Sources: AllAfrica, Aspen Institute, CNN, IRIN, RH Reality Check, U.S. Department of State, USAID.
Photo Credit: United Nations Photo. -
Nancy Lindborg, The Huffington Post
For Yemen’s Future, Global Humanitarian Response Is Vital
›June 12, 2012 // By Wilson Center StaffThe original version of this article, by Nancy Lindborg, appeared on The Huffington Post.
This weekend in Sana’a, I had dinner with a group of young men and women activists who are on the forefront of Yemen’s historic struggle for a better future. They turned out for change with great courage last year, and at dinner, with great eloquence they outlined for me the many challenges facing Yemen during this critical transition period: conflict in the north and south, weak government institutions, cultural barriers to greater women’s participation, an upended economy, and one of the world’s highest birthrates. And, as one man noted, it is difficult to engage the 70 percent of Yemeni people who live in rural areas in dialogue about the future when they are struggling just to find the basics of life: food, health, water.
His comment makes plain the rising, complex humanitarian crisis facing Yemen. At a time of historic political transition, nearly half of Yemen’s population is without enough to eat, and nearly one million children under the age of five are malnourished, putting them at greater risk of illness and disease. One in 10 Yemeni children do not live to the age of five. One in 10. This is a staggering and often untold part of the Yemen story: a story of chronic nationwide poverty that has deepened into crisis under the strain of continuing conflict and instability.
Unfortunately, in communities used to living on the edge, serious malnutrition is often not even recognized in children until they are so acutely ill that they need hospitalization.
Continue reading on The Huffington Post.
Nancy Lindborg is the assistant administrator of the Bureau for Democracy, Conflict, and Humanitarian Assistance at the U.S. Agency for International Development.
Sources: U.S. Department of State.
Photo Credit: Informal settlements near the Haddjah governorate, courtesy of E.U. Humanitarian Aid and Civil Protection.
Showing posts from category USAID.