Showing posts from category global health.
-
USAID Egypt’s Health and Population Legacy Review
›On May 23 the Middle East Program, ECSP, and the Global Health Initiative of the Woodrow Wilson Center, along with the Global Health Technical Assistance Project, hosted a panel of speakers discussing the past 30 years of the U.S. Agency for International Development’s health and population initiatives in Egypt, as outlined in the new Egypt Health and Population Legacy Review. Geoffrey Dabelko, director of ECSP and coordinator of the Global Health Initiative at the Wilson Center, moderated the event. [Video Below]
Peter McPherson, former administrator of USAID during the Reagan administration, and George Laudato, the administrator’s special assistant for the Middle East, presented on the historical context behind USAID in Egypt and the results of their efforts. McPherson pointed to three lessons that can be drawn from the recent report:- “Big payoffs” require long-term efforts; and
- Economic support for a country can have a dramatic impact; but
- The host country’s commitments and investments are still important.
Motaz Zahran, political counselor for the Embassy of Egypt, noted that USAID efforts were “just one sector of a fruitful partnership” between the United States and Egypt that he hoped would continue. He said the success story outlined by the report was reflective of improvements in coordination and addressing specific goals.
Other panelists outlined the successes of USAID in Egypt as related to their own areas of expertise. Leslie B. Curtin, co-author of the review and an expert in demographics and health outcomes, noted the dramatic improvements in a range of health sectors, in particular the rise in contraceptive prevalence and immunization rates and decrease in both maternal and infant mortality rates.
Nahed Matta, MD, senior maternal and newborn health officer at USAID, focused on improvements to the quality of maternal health, which she said were made possibly through better technology and increased fact-gathering to identify the key factors regarding maternal health trends. Sameh El-Saharty, MD, senior health policy specialist at the World Bank and Health Legacy Review Committee member, credited the increased number of health professionals in Egypt, better information gathering on health systems, and restructured models of health insurance, as successful strategies.
Concluding the session, Amie Batson, deputy assistant administrator for Global Health at USAID, discussed the lessons that other development initiatives can draw from the legacy of USAID efforts in Egypt. She highlighted the importance of country ownership, in which the developing country engages with other institutions and religious and political leaders at both national and local levels, and of policies that fund routine monitoring and evaluation. She also outlined the possibilities of innovation and south-to-south sharing on the local and international scale, referencing inroads made by two recent initiatives: the “MAMA” mobile device program, launched by Secretary Clinton in May 2011 to assist with disseminating maternal health information, and the Saving Lives at Birth initiative, launched by USAID in partnership with several other organizations in March 2011.
Laura Rostad is an intern for the Middle East Program at the Woodrow Wilson Center.
Image Credit: Adapted from cover of the Egypt Health and Population Legacy Review, courtesy of USAID; cover photo courtesy of Leslie Curtin. -
Family Planning as a Strategic Focus of U.S. Foreign Policy
›May 11, 2011 // By Wilson Center Staff“Family Planning as a Strategic Focus of U.S. Foreign Policy,” by Elizabeth Leahy Madsen, was an input paper for the Council on Foreign Relations report, The Role of U.S. Family Planning Assistance in U.S. Foreign Policy. Excerpted from the introduction:
Comprehensive policies that incorporate demography, family planning, and reproductive health can promote higher levels of stability and development, thereby improving the health and livelihood of people around the world while also benefiting overarching U.S. interests. U.S. foreign aid will be more effective if increased investments are made in high population-growth countries for reproductive health and family planning programs. These programs are cost-effective because they help reduce the stress that rapid population growth places on a country’s economic, environmental, and social resources.
Family Planning and Reproductive Health Programs
Family planning and reproductive health programs have successfully reduced the world’s population growth rate, propelled economic development, and improved women’s lives across the world. When people, and especially women, are given the opportunity and technology to limit their family size, they often choose to do so.
Population trends are motivated by three demographic forces: fertility, mortality, and migration. Although they can have dramatic effects on national and local populations, mortality and migration in particular have relatively little influence globally. Across the world, mortality rates have declined to a point where most children born today live to reach their own reproductive years, though much work remains to reduce the effect of communicable diseases and improve nutrition among the young. Meanwhile, three percent of the world’s population currently lives outside of their birth-countries. Therefore, while migration is increasing and an important demographic force, it does not occur at a scale large enough to significantly affect global-level demography.
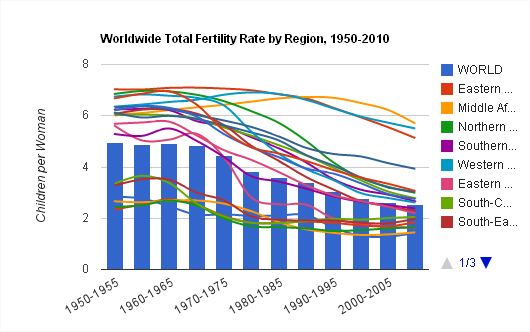
Fertility rates currently are – and in the short-term will remain – the most important driver of global demographic trends. The total fertility rate, or average number of children born to each woman, has been estimated at 2.7 for the period between 2000 and 2005, a decline from 3.6 children per woman in the early 1980s. Given this decline, population projections generally assume future declines in fertility rates. For example, the widely cited “medium-fertility variant,” which is the United Nations’ projection of a world population growing from 6.9 billion in 2010 to 9.1 billion by 2050, relies upon an assumption that the global fertility rate will decline by 24 percent to two children per woman. However, if fertility rates remain constant at current levels, the world’s population would reach 11 billion by 2050. Fertility rates, whether they decline or remain at current levels, are not distributed evenly among countries and regions.
Continue reading or download the full report, “Family Planning as a Strategic Focus of U.S. Foreign Policy,” from the Council on Foreign Relations. -
Isobel Coleman, Council on Foreign Relations
Report: Family Planning and U.S. Foreign Policy
›May 10, 2011 // By Wilson Center StaffThe original version of this brief, by Isobel Coleman of the Council on Foreign Relations, is based on the report, Family Planning and U.S. Foreign Policy: Ensuring U.S. Leadership for Healthy Families and Communities and Prosperous, Stable Societies, by Isobel Coleman and Gayle Lemmon.
Click here for the interactive version (non-Internet Explorer users only).
U.S. support for international family planning has long been a controversial issue in domestic politics. Conservatives tend to view family planning as code for abortion, even though U.S. law, dating to the 1973 Helms Amendment, prohibits U.S. foreign assistance funds from being used to pay for abortion. Indeed, increased access to international family planning is one of the most effective ways to reduce abortion in developing countries. Investments in international family planning can also significantly improve maternal, infant, and child health. Support for international voluntary family planning advances a wide range of vital U.S. foreign policy interests – including the desire to promote healthier, more prosperous, and secure societies – in a cost-effective manner.
Saving Lives of Mothers and Children
More than half of all women of reproductive age in the developing world, some 600 million women, use a form of modern contraception today, up from only 10 percent of women in 1960. This has contributed to a global decline in the average number of children born to each woman from more than six to just over three. Despite these gains, an estimated 215 million women globally – particularly in sub-Saharan Africa and southern Asia – are sexually active but are not using any contraception, even though they want to avoid pregnancy or delay the birth of their next child. With the world’s population poised to cross the seven billion mark later in 2011, and expected to grow by nearly 80 million people annually for several more decades, global unmet need for family planning is likely to increase.
Studies have shown that contraception could reduce maternal deaths by a third, from approximately 360,000 to 240,000; reduce abortions in developing countries by 70 percent, from 35 million to 11 million; and reduce infant mortality by 16 percent, from 4 million to around 3.4 million.
For a woman in the developing world, the lifetime risk of dying from pregnancy is still one of the greatest threats she will face. In developed countries, 1 out of 4,300 women will lose her life as a consequence of pregnancy, compared to sub-Saharan Africa, where that figure soars to 1 in 31, and Afghanistan, where the lifetime risk of dying from pregnancy is 1 out of 7.
Unsafe abortions are one factor contributing to high maternal death rates. As of 2008, 47,000 abortion-related maternal deaths occur annually, accounting for 13 percent of all maternal deaths. Filling the unmet need for modern family planning would lead to a reduction in mistimed pregnancies and a significant decline in abortions and abortion-related health complications. In 2000 alone, if women who wished to postpone or avoid childbearing had access to contraception, approximately 90 percent of global abortion-related and 20 percent of obstetric-related maternal deaths could have been averted.
Maternal mortality has a devastating and irreversible effect on children and families. Indeed, countries with the highest maternal mortality rates also experience the highest rates of neonatal and childhood mortality. When a mother dies, her surviving newborn’s risk of death increases to 70 percent.
Family planning presents an opportunity to curb maternal and under-five deaths not simply by giving women of all ages the ability to determine their family size, but by enabling women to delay pregnancy until at least age 18 and to space and plan their births. In this way, modern contraceptive methods help women avoid high-risk pregnancies. Studies suggest that short pregnancy intervals (when the pregnancy occurs less than twenty-four months after a live birth) are associated with an increased risk of maternal and under-five mortality. In fact, if all mothers were to wait at least 36 months to conceive again, it is estimated that 1.8 million deaths of children under five could be prevented annually.
Enhancing International Security
While much of the developed world is experiencing population stability or even decline, many countries in the developing world continue to see rapid population growth. Population imbalances have emerged as a serious issue affecting economic opportunity, global security, and environmental stability. Ongoing civil conflicts, radicalism, weak governance, and corruption are endemic problems for many fragile states. While high fertility rates are not the cause of their problems, they do complicate the challenges these countries face in trying to reduce poverty, achieve per capita income growth, provide education and productive opportunities for youth, and address increasing shortages of natural resources.With the world’s population poised to cross the 7 billion mark later in 2011, and expected to grow by nearly 80 million people annually for several more decades, global unmet need for family planning is likely to increase.
Yemen, for example, has the highest rate of unmet need for family planning of any country. Its population has doubled in less than 20 years, and it has the world’s second-youngest population. High fertility – around six children per woman – taxes Yemen’s infrastructure, education and health systems, and environment. In addition, its labor force is growing at a pace much faster than the growth of available jobs, resulting in high youth unemployment. Increasing access to family planning would help improve Yemen’s long-term prospects for achieving per capita growth and stability. Conversely, continued high fertility rates will only deepen Yemen’s current crises.
Many countries experiencing fast population growth – like Yemen – do not have the capacity to harness the potential of their young populations. In these cases, high fertility rates can lead to a vicious cycle of poverty at the community, regional, and national levels. Rapidly growing populations are also more prone to outbreaks of civil conflict and undemocratic governance. Eighty percent of all outbreaks of civil conflict between 1970 and 2007 occurred in countries with very young populations. Demographers have shown that the statistical likelihood of civil conflict consistently decreases as countries’ birth rates decline.
Countries with the highest population growth rates face real resource constraints, particularly arable land and clean water. As of 2010, 40 percent of populations in more than 35 countries have insufficient access to food, with the largest concentration in central and eastern sub-Saharan Africa. Given that many of these food-insecure countries will continue to experience significant population growth in decades ahead, malnutrition will remain a challenge.
Continue reading at the Council on Foreign Relations or download the full report, Family Planning and U.S. Foreign Policy: Ensuring U.S. Leadership for Healthy Families and Communities and Prosperous, Stable Societies.
Isobel Coleman is a senior fellow for U.S. foreign policy; director of the Civil Society, Markets, and Democracy Initiative; and director of the Women and Foreign Policy Program at the Council on Foreign Relations.
Sources: Council on Foreign Relations, Population Action International, Population Reference Bureau, UNFPA, World Health Organization.
Chart Credit: Arranged by Schuyler Null, data from UN Population Division, World Population Prospects, 2010 Revision. -
Reporting on Global Health: A Conversation With the International Reporting Project Fellows
›“The story is the story, the information is the information, but you can frame it in very different ways,” said freelance journalist Annie Murphy at a roundtable discussion on the current state of global health reporting. Fresh off their five-week assignments, Murphy and three other fellows from the International Reporting Project (IRP) – Jenny Asarnow, Jill Braden Balderas, and Ann S. Kim – spoke at an event at the Woodrow Wilson Center on April 28 about their experiences researching underreported health issues in Haiti, Botswana, Mozambique, and Uganda. [Video Below]
Taking the Temperature of Global Health Reporting
Global health reporting, like many other forms of journalism, has felt the pinch from the global financial crisis, said Balderas, who edited a recent Kaiser Foundation report on the issue, “Taking the Temperature: The Future of Global Health Journalism.” Other challenges that have led to less global health coverage in mainstream media include an increased focus on “hyper-local” news; “story fatigue” from years of HIV/AIDS coverage; greater focus on epidemics and disasters; and the increasing number of advocacy groups starting their own news services.
Placing global health stories is a big challenge, agreed all four panelists. Who will want to run the story? What form – radio, documentary, print, online – will the story take? According to Murphy, some creative thinking may be needed: “It is global health, but that doesn’t mean we always have to frame it in this box of global health. It will be global health no matter what we do, so I think it’s also important for us to feed it into other events and issues that are important.”
(Re)building Maternal Healthcare in Haiti
With the worst maternal and infant mortality rates in the Western Hemisphere, Haiti needs medical providers of all kinds, said Asarnow, but especially skilled birth attendants. The devastating earthquake in 2010 destroyed Haiti’s only midwifery school, located in Port-au-Prince, killing many students and instructors. The school is still struggling to graduate a class of 15 people, she said.
In the rural town of Hinche, located in Haiti’s Central Plateau region, Asarnow frequently visited a public hospital that provided pregnant women with free obstetric care. Yet, she said, “even with free care, there [were] still a lot of barriers for women coming to the hospital to get care.” For example, the family members of expectant mothers had to provide sheets, clothing, food, and a bucket for personal needs. In addition, some women were too poor to afford transportation to and from the hospital.
Most women in Haiti, though, give birth at home with the help of traditional birth attendants, called matrones, Asarnow said. These matrones, popular in rural areas, are not formally educated in midwifery, but the government, along with non-profits such as Midwives for Haiti, have provided the matrones with training in basic health care and emergency situations.
Simply reporting on childbirth turned out to be a challenge, said Asarnow. “It’s hard to get people interested in something that just happens to most women,” she said; other more unusual health problems, such as infectious diseases, tend to garner more interest.
Finding Health Sovereignty in Mozambique
Health sovereignty, explained Murphy, is “the idea that nations have the right to make decisions about health and about how people are going to be treated” – an issue that is particularly pointed in Mozambique, where 50 percent of the national budget and 70 percent of the annual health budget is tied to international aid.
Mozambique, said Murphy, has only 1,000 doctors to serve a population of 22 million. By contrast, the country has an estimated 50,000 traditional healers. As a result, she said, most Mozambicans use traditional healing for at least part of their regular health care.
While researching traditional healers in the northern province of Tete, Murphy investigated a large Brazilian-owned coal mine that had displaced 5,000 local people when it was built. Mining is a major economic activity in Mozambique, yet mining companies are taxed a mere three percent by the government, said Murphy.
Health reporting doesn’t have to only cover traditional health issues, said Murphy. “The environment, natural resources, and how a country earns its money very much have to do with the health of the people who are living there,” she said. “How can you talk about being sovereign and providing health to your citizens if you don’t have the money to do that?”
Treating the Over-Treatment of Malaria in Uganda
“Malaria is quite over-treated” in Uganda, said Balderas. There’s the “idea that if you have a fever, you have malaria.” Consequently, the rate of misdiagnosis can reach alarming rates in some areas, she said.
Balderas said an estimated 50 percent of Ugandans get free treatment through the public sector. However, only donor-funded facilities are equipped with the rapid diagnosis test (or RDT), which takes only 20 minutes to determine the presence of malaria in a blood sample, she said. If these facilities were more widespread, misdiagnoses rates could easily be lowered.
Other challenges to the accurate diagnosis and treatment of malaria include faulty equipment, shortages of electricity and lab technicians, human error, corruption, bureaucratic entanglements, and presumptive diagnoses. For example, sometimes health workers do not know what is causing a patient’s fever, Balderas said, but they prescribe malaria treatments anyway because “they want to be able to give someone a treatment; they want to feel like they’re helping people.”
“There are certainly a ton of issues that relate to health,” Balderas said, such as poverty and corruption. Everyone she interviewed in Uganda – with the exception of government officials – identified the corruption in the country’s drug sector as a key problem.
Helping “Africa” One Small Story at a Time
Inspired by a World Health Organization study, which found “at least a 60 percent reduction in HIV infection among men who were circumcised,” Kim went to Botswana to investigate infant circumcision, a practice that is gaining popularity but is still alien. “I would meet people in the course of my day and they would ask me what I was doing there and I would talk about circumcision. They’d say, ‘Oh, I really want to get my baby circumcised. How do I do that?’” she reported.
The most powerful moment of her trip, said Kim, came when she was researching cervical cancer – the number one cancer among women in Botswana. As she waited with a woman to receive her lab results, Kim asked her if she was nervous. The woman, who was HIV-positive, said, “Yeah, I’m really worried. To me, it would be worse to get cervical cancer than to have HIV.” Even though Botswana is a middle-income country, said Kim, there are far more resources available to treat HIV than cancer.
Kim said that when presenting her work it was important for her to bring in the human element and not just the statistics: “I hope that, in whatever small way, even these small stories will help get issues in various countries on the map, especially in Africa where we tend to think of it as ‘Africa’ and not so much as different countries with different personalities and different situations.”
Sources: Malaria Journal, UNFPA, World Health Organization.
Image Credit: David Hawxhurst/Woodrow Wilson Center. -
Designing Health and Population Programs to Improve Equity: Moving Beyond the Rhetoric
›“There needs to be ongoing flexibility and creativity in our ways of approaching health equity,” said John Borrazzo of the U.S. Agency for International Development (USAID) at a recent Global Health Initiative event at the Wilson Center. Borrazzo is the chief of the Maternal and Child Health Division in the Bureau for Global Health. He moderated a discussion on practical strategies to improving access to health services for the world’s poor and other marginalized groups, with panelists Mickey Chopra, chief of health and associate director of programmes at UNICEF; Davidson Gwatkin, senior fellow at the Results for Development Institute and senior associate at Johns Hopkins Bloomberg School of Public Health; Cesar Victoria, professor of epidemiology at the Federal University of Pelotas in Brazil; and Jennifer Luna, senior monitoring and evaluation adviser for the Maternal and Child Health Integrated Program (MCHIP). [Video Below]
MDG 4: An Equity Approach
“Massive benefits can be gained by reaching the poorest and most marginalized,” said Chopra. “It’s actually more cost effective to have an equity-based approach; it’s not just right in principle, it’s right in practice.”
While there has been some progress in reducing the rates of mortality for children under five (the UN’s Millennium Development Goal 4), Chopra said “there has to be a change” if they are going to be achieved completely. Most of the 30 percent decline in child mortality so far has been in Asian countries, while Africa as a whole remains stagnant. Further, two-thirds of the 35 countries that have made significant progress to meet MDG 4 show worsening inequalities between the highest and lowest income brackets of the population.
In the majority of countries, the “rich are still capturing most of the benefits of new investments and interventions,” said Chopra. “The challenge at the program and policy levels is to understand why there is this gap between the richest and the poorest in terms of uptake of critical interventions.”
Delivery channels are faced with “bottlenecks” that prevent services from reaching marginalized communities, said Chopra. Clinic-based services often lack adequate human resources, consistency in the quality of service, and can be very expensive. Population-oriented services, which include government and NGO-led outreach and scheduled services at health facilities, are often challenged with low demand and lack of continuity, while availability and cost of health commodities are barriers for community-based interventions delivered through local organizations or social marketing campaigns.
Shifting delivery of services within channels, appropriately shifting delivery to different channels, or improving the performance of an established delivery channel could help increase uptake of treatment and prevention among poor and marginalized communities, concluded Chopra. He stressed that progress need not come at the expense of the poor. According to a UNICEF report, Ghana, Eritrea, Nepal and Malawi have all reduced under-five mortality and inequality by prioritizing providing essential services to the most marginalized communities first.
Designing Equity-Based Health Programs
“Performance variability in terms of equity across countries is very large,” said Gwatkin. “In some places a given technique can work well and in others it can be a complete flop.”
To pick the right technique for the right place, Gwatkin advocated for an iterative approach to program design and implementation, beginning with setting targets in terms of the poor population group of concern. After fully assessing country-specific conditions, a set of potential pro-poor interventions can be selected, based on an analysis of current interventions and suggested alternatives as well successful interventions in other countries. Each of these interventions should be delivered to a large, representative area, he said.
“The next step is to find out how well you have done,” said Gwatkin, stressing the importance of assessing and monitoring interventions with a specific focus on the marginalized target group. Successful approaches should be expanded, while those that are not having the intended benefits of helping the poorest communities should be modified or abandoned.
In sum, said Gwatkin, “It’s more promising to focus on designing a process to fit techniques to individual country settings than to focus on the techniques themselves.” Doing this helps effectively integrate equity concerns into the design and implementation of programs, and as a result, he said, can have a major impact on improving the lives of the poorest people in developing countries.
Analyzing Equity to Maximize Impact
“It’s always possible and useful to include equity in monitoring and evaluation, however, it has to be planned ahead of time,” said Victoria.
The Countdown to 2015 Initiative is an effort to monitor progress made towards the health-related Millennium Development Goals globally. The Countdown’s efforts not only aim to promote access to health services at the aggregate level but also specifically to ensure the equitable distribution and uptake of health services among disadvantage populations, said Victoria.
Generally, in countries with high coverage of preventative and treatment services, like Brazil, there is “bottom inequity,” said Victoria, in which the poor are much worse off than everyone else. Targeting the poor specifically in such countries is therefore essential to improving equity.
Alternately, Victoria continued, countries with low coverage at all levels, like Cambodia or Haiti, suffer from “top inequity,” in which the rich are typically much better off the rest of the population. These countries should work towards increasing coverage for all people and focus on the poor after there are some universal gains, he said.
“Analyzing the shapes of inequity curves can help drive decisions about delivery channels and targeting…and can lead to practical strategies for maximizing the impact of interventions,” concluded Victoria.
Health Equity: From Evidence to Practice
“Projects often state that they are really interested in equity, but when you read the project descriptions, you don’t see exactly what they mean by equity or how they plan on addressing it,” said Luna, speaking of her work at MCHIP.
Luna presented the Health Equity Guidance Document that outlines a systematic, six-step process for professionals who design and implement community-oriented projects to ensure equity is effectively integrated into their programs:1) Understand the equity issues in the project area
Luna stressed that there is no “one size fits all” strategy: “This approach is not a prescriptive one; it presents a series of concepts and approaches to take into consideration and then make decisions.” But for program implementers on the ground, she said, these guidelines and tools “should help lead to a coherent health equity strategy and can serve as a basis for dialogue among stakeholders.”
2) Identify the disadvantaged group on which to focus
3) Decide what is in the project’s manageable interest to change
4) Define equity goals, objectives, and a project-specific definition of equity
5) Determine equity strategies and activities
6) Develop equity-focused monitoring and evaluation
Sources: UNICEF, United Nations Development Programme, World Health Organization.
Image Credit: “Malaria prevention, Kenya,” courtesy of flickr user DFID. -
Accessing Maternal Health Care Services in Urban Slums: What Do We Know?
›“Addressing the needs of urban areas is critical for achievement of maternal health goals,” said John Townsend, vice president of the Reproductive Health Program at the Population Council. “Just because there is a greater density of health services does not mean that there is greater access.”
Townsend moderated a discussion on the challenges to improving access to quality maternal health care in urban slums as part of the 2011 Maternal Health Dialogue Series with speakers Anthony Kolb, urban health advisor at USAID; Catherine Kyobutungi, director of health systems and challenges at the African Population Health Research Center; and Luc de Bernis, senior advisor on maternal health at the United Nations Population Fund (UNFPA). [Video Below]
Mapping Urban Poverty
“Poverty is becoming more of an urban phenomenon every day,” said Kolb. With over 75 percent of the poor in Central Asia and almost half of the poor in Africa and Asia residing in cities and towns by 2020, “urban populations are very important to improving maternal health,” he added.
Collecting accurate data in informal settings such as slums can be very challenging, and there is often a “systematic undercounting of the urban poor,” said Kolb. Data often fails to capture wealth inequality in urban settings, and there is often a lack of attention to the significant variability of conditions between slums.
Kolb also warned about the risk of generalization: “Slums and poverty are not the same.” In practice, there is not a standardized definition of what constitutes a slum across countries, he said. “It is important to look at different countries and cities individually and understand how inequality is different between them.” Slum mapping can help to scope out challenges, allocate resources appropriately, and identify vulnerability patterns that can inform intervention design and approach, he said.
Maternal Health in Nairobi Slums
Addressing the maternal health needs of the nearly 60 percent of urban residents who live in slums or slum-like conditions will be a critical step to improving maternal health indicators of a rapidly urbanizing Kenya, said Kyobtungi.
Only 7.5 percent of women in Kenyan slums had their first antenatal care visit during their first trimester of pregnancy and only 54 percent had more than three antenatal care visits in all – rates significantly lower than those among urban women in non-slum settings.
“In some respects, [the urban poor] are doing better than rural communities, but in other ways they are behind,” said Kyobtungi. But, she said, there are many unique opportunities to improve maternal health in slums: “With these very high densities, you do have advantages; with very small investments, you can reach many more people”
Output-based voucher schemes – in which women pay a small fee for a voucher that entitles them to free, high-quality antenatal care, delivery services, and family planning – have been implemented to help poor, urban women access otherwise expensive services. But poor attitudes towards health care workers, transportation barriers, and high rates of crime still prevent some women from taking advantage of these vouchers, said Kyobtungi.
The majority of maternal health services in slums are provided by the private facilities, though size and quality vary widely. “There is a very high use of skilled attendants at delivery, but the definition of skilled is questionable,” said Kyobtungi
“Without supporting the private sector,” Kyobutungi said, “we cannot address the maternal health challenges within these informal settlements.” Combined with an improved supervision and regulation system, providing private maternal health facilities with training, equipment, and infrastructure could help to improve the quality of services in urban slums, she concluded.
Reducing Health Inequalities
“While we have evidence that health services, on average, may be better in urban areas than in rural areas, this often masks wide disparity within the population,” said de Bernis. “Reducing health inequities between and within countries is a matter of social justice.”
When it comes to family planning, total fertility rates are lower in cities, but “the unmet need…is still extremely important in urban areas,” explained de Bernis. Many poor women in cities, especially those who live in marginalized slum populations, do not have access to quality reproductive health services – a critical element to reducing maternal morbidity and mortality rates.
Economic growth alone, while important to help improve the health status of the poor in urban settings, will not solve these problems, said de Bernis. To reduce health disparities within countries, de Bernis advocated for “appropriate social policies to ensure reasonable fairness in the way benefits are distributed,” including incorporating health in urban planning and development, strengthening the role of primary health care in cities, and putting health equity higher on the agenda of local and national governments.
Event Resources:Source: African Population Research Center, United Nations Population Fund.
Photo Credit: “Work Bound,” courtesy of flickr user Meanest Indian (Meena Kadri). -
Marissa Mommaerts, Aspen Institute
Aspen Institute: The Revolution We Need in Food Security and Population
›April 27, 2011 // By Wilson Center StaffThe first months of this year brought the second global food price crisis in just three years, with soaring food prices against a backdrop of bad weather, poor harvests, and political turmoil in North Africa and the Middle East. This year will see another milestone: the planet’s population is set to surpass seven billion, with most of the population growth occurring in countries least equipped to meet rising demands on agriculture and the environment. As part of its 7 Billion: Conversations that Matter roundtable series, the Aspen Institute’s Global Health and Development Program brought together three experts to discuss “The Revolution We Need in Food Security and Population” on April 12.
-
Population Growth and its Relation to Poverty, the Environment, and Human Rights
›“Population, Poverty, Environment, and Climate Dynamics in the Developing World,” in the Interdisciplinary Environmental Review, by Jason Bremner, David Lopez-Carr, Laurel Suter, and Jason Davis, attempts to illuminate and clarify the complex relationships between environmental degradation, population dynamics, and poverty. Population growth is a key driver for the degradation of ecosystem services which has a direct impact on livelihoods and human well-being, write the authors, especially for the poor. They argue that “population growth itself, however, remains an insufficient explanation of the relationship between population, ecosystems, and poverty.” While the field has a come a long way since its “original Malthusian roots,” they write, the relationships between these dynamics differ greatly depending on the area in question, and much work remains to be done on the less well-studied ecosystems.In “An End to Population Growth: Why Family Planning Is Key to a Sustainable Future” from the Solutions Journal, Robert Engelman reminds us that population projections are not set in stone and that the widespread belief that population has to reach nine billion before leveling off is wrong. Nor is coercive “population control” necessary, he writes: “Population growth rates and average family size worldwide have fallen by roughly half over the past four decades, as modern contraception has become more accessible and popular.” Unfortunately, there remains a large number of people around the world without access to family planning, the majority of whom live in developing countries. Engelman points out that while the number of people of reproductive age has steadily increased in these countries over the last decade, donor support has declined. He argues that research, courage, and creativity are needed to reverse this situation, but in a world where most of all pregnancies were intended, population growth would slow long before reaching nine billion.