
Showing posts from category global health.
-
Population, Health, and Environment
›The WWF and Equilibrium Research released a report on the interplay between the environment and human health. Vital Sites: The Contribution of Protected Areas to Human Health documents the environmental-human health connection, provides case studies from both the developed and developing worlds, and offers recommendations to enhance the health outcomes that can be gained from environmental good governance. “[P]rotected areas are not a luxury but are key sites to protect not only biodiversity, but also ecosystem services and our wider well-being,” the World Bank’s Kathy MacKinnon writes in the foreword. “Family Planning and the Environment: Connected Through Human and Community Well-Being,” part of PATH‘s Outlook series, details the importance of family planning-environmental projects to communities living in remote and ecologically vulnerable areas. Designed for practitioners, the article aims to promote cross-discipline dialogue and offers case studies from the Philippines and Uganda. The article concludes that “more collaborative family planning and environmental efforts aimed at reducing inequities would better ensure sustainable community development as well as the right of individuals to achieve what they value.”
“Family Planning and the Environment: Connected Through Human and Community Well-Being,” part of PATH‘s Outlook series, details the importance of family planning-environmental projects to communities living in remote and ecologically vulnerable areas. Designed for practitioners, the article aims to promote cross-discipline dialogue and offers case studies from the Philippines and Uganda. The article concludes that “more collaborative family planning and environmental efforts aimed at reducing inequities would better ensure sustainable community development as well as the right of individuals to achieve what they value.” -
To Invest in a Sustainable Future, Fund Voluntary Family Planning
›President Obama’s proposed federal budget for FY2011 includes $715.7 million for international family planning and reproductive health assistance—10 percent ($67 million) more than what was included in the FY2010 budget that Congress approved last December. If approved, the FY2011 allocation would be 54 percent more than the FY2008 budget, which was equivalent to the amount allotted in 1974 when adjusted for inflation. The recent increases mark the end of more than 30 years of stagnation in U.S. funding for voluntary family planning—and herald a new investment in a sustainable future.
Over the last 20 years, the number of women of reproductive age in the developing world has increased by 465 million. Today, the Guttmacher Institute estimates that 201 million women in developing countries want but lack access to modern contraceptives. “Satisfying the unmet need for contraceptive services in developing countries would avert 52 million unintended pregnancies annually, which, in turn, would save more than 1.5 million lives and prevent 505,000 children from losing their mothers,” the Institute reports.
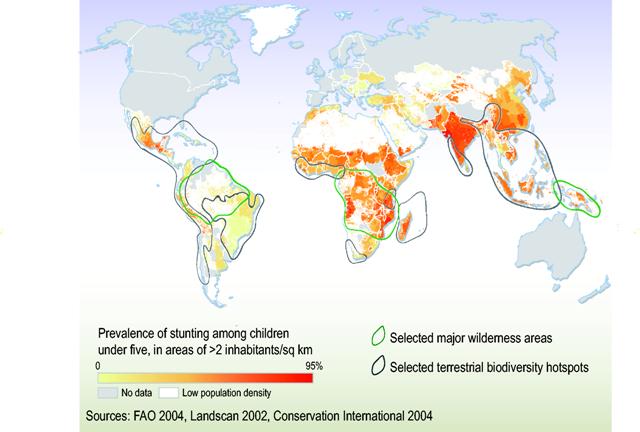
Rapid population growth in some of the world’s most economically disadvantaged countries poses a significant threat to their natural resources and the environment. Currently, more than 1 billion people live in ecological hotspots—areas that are both rich in plant and animal diversity and highly threatened by human activity. Although these areas comprise just 12 percent of the Earth’s land surface, they hold nearly 20 percent of the global population and possess a population growth rate nearly 40 percent greater than the world average. The cumulative impact of a growing global population, which demands more natural resources and exacerbates already unsustainable patterns of consumption, degrades the most basic foundations of life—air, water, croplands, forests, and fisheries—and contributes to climate change.
Improving access to voluntary family planning not only contributes to smaller, healthier families, but also eases the strain on natural resources. By giving couples the information and supplies to plan the number and timing of their children, U.S.-funded population and reproductive health programs have helped countries slow population growth and reduce population pressures on finite natural resources, including local habitats and wildlife. In addition, the success of USAID’s population, health, and environment programs also offers important lessons for climate change adaptation and building resilience in local communities.
In our interconnected environment, the impacts of natural resources use, management, and protection around the world are felt here in the United States. Despite the difficult budgetary and economic environment our country faces, the president’s request for approximately $716 million in international family planning and reproductive health assistance funding is a wise long-term investment. These resources are an important step toward the broader goal of investing $1 billion in these critical programs to create a healthier, more sustainable future for our world.
Rebecca Wadler Lase is the program associate for the Sustainability Education Program at the Izaak Walton League of America.
Map: “Poverty-Biodiversity Mapping Applications.” Courtesy UNEP/Grid Arendal. -
Canada Flip-Flops on Family Planning, Will the G-8 Follow?
›April 5, 2010 // By Laura Pedro“The Canadian government should refrain from advancing the failed right-wing ideologies previously imposed by the George W. Bush administration in the United States, which made humanitarian assistance conditional upon a ‘global gag rule’ that required all non-governmental organizations receiving federal funding to refrain from promoting medically-sound family planning,” said the Canadian Liberal Party about the country’s Conservative government in a Parliamentary motion last week.
Though Prime Minister Stephen Harper had pledged to include a voluntary family planning initiative in Canada’s foreign aid plan at last year’s G8 meeting in Italy, the Conservative government recently said that the initiative will not be part of its G8 plan at the upcoming meeting in Canada this June.
This move has surprised both Canadians and Americans. U.S. President Obama overturned the Mexico City policy last year, and has fully supported the inclusion of family planning methods as part of foreign aid.
Harper’s government has maintained that maternal and child health services, such as vaccinations and nutrition, will be a priority, but various components of family planning, including birth control and abortion, will not be included in the Canadian initiative.
The Tories, as along with three Liberal MPs, voted down the Liberal motion 138-144, which requested clarification of Harper’s maternal health initiative and pushed for the inclusion of the full range of family planning options. The Tories focused solely on what they called “anti-American rhetoric” in the motion, which drew attention away from the divisive issue of abortion.
The issue has got caught up in domestic Canadian politics, with opposition Liberals trying to equate the Conservatives with the George W. Bush administration and the Conservatives trying to avoid discussion of intra-party debates on the contentious issue of abortion.
Now it seems likely like that Harper will go to the G8 summit in Ontario with a foreign aid plan for maternal health that makes no reference to issues of contraception. According to Canada’s International Co-operation Minister Bev Oda, “saving lives” of women and children is a higher priority than family planning.
But most international maternal health advocates don’t agree. “Maternal mortality rates are high among women who do not have access to family planning services. Contraception can reduce the number of unplanned pregnancies,” said Calyn Ostrowski, program associate for the Wilson Center’s Global Health Initiative. “For example, at a recent event on our Maternal Health series, Harriet Birugni of the Population Council in Kenya described how integrating reproductive health services such as family planning can reduce maternal mortality rates, particularly for poor young women who have the least access to contraception.”
In response to Canada’s announcement, U.S. Secretary of State Hilary Clinton said that the United States will be promoting global health funding, including access to contraception and abortion, at the G8. “You cannot have maternal health without reproductive health,” she said during a news conference with other G8 ministers. Britain has also agreed with this position, which has led Canadian Liberal Party Leader Michael Ignatieff to say that Canada’s G8 position goes against the international consensus.
Laura Pedro is the program assistant for the Canada Institute, and a graduate of the University of Vermont.
Photo.: Prime Minister Stephen Harper, courtesy Flickr user Kashmera -
Maintaining the Momentum: Highlights From the Uganda International Conference on Family Planning
›“Family planning is to maternal survival what a vaccination is to child survival,” said Johns Hopkins professor Amy Tsui, quoting Khama Rogo of the World Bank, at the Woodrow Wilson Center event Maintaining the Momentum: Highlights From the Uganda International Conference on Family Planning on March 16. Rogo made the strong statement during the landmark November 2009 conference in Kampala, which has renewed interest in family planning and reproductive health among African leaders and development partners. Rhonda Smith of the Population Reference Bureau and Sahlu Haile of the David and Lucile Packard Foundation joined Tsui, the director of The Bill & Melinda Gates Institute of Population & Reproductive Health, to discuss their impressions of the Kampala conference and what it means for the future of family planning in Africa.
“An event that happened at the right time”
“Kampala was the work of a community,” said Tsui. More than 50 organizations—the U.S. Agency for International Development, the UN Population Fund, the World Bank, the World Health Organization, and the Gates and Packard Foundations—convened in Uganda, which was chosen not only for its central location, but also to highlight the country’s soaring unmet need for contraception—41 per cent—and rapid 3.1 percent population growth rate.Panels focused on key issues in family planning, including:- Integrating family planning into HIV/AIDS care
- Integrating family planning in post-abortion, postpartum, child, and other primary health care
- Expanding contraception delivery services by community health workers
- Increasing outreach to youth and men
- Capitalizing on private and public innovations in service delivery and financing
- The United States announced its foreign assistance budget will increase support for family planning from $450 million to $715 million for the next fiscal year.
- The Global Health Initiative identified maternal/child health and family planning as one of its main priority themes.
- Secretary of State Clinton positively discussed girls’ education, family planning, and reproductive health at the ICPD + 15 anniversary.
- The Women Deliver 2010 Conference, to be held in June, has identified family planning as a third pillar of maternal health.
Uganda on the MoveRhonda Smith’s presentation “Uganda on the Move”—which she also presented in Uganda—is a prototype of the Population Reference Bureau’s new ENGAGE (Eliminating National Gaps—Advancing Global Equity) project, which is designed to “engage policy audiences and promote policy dialogue around issues of high fertility and high unmet need for family planning and their costs, consequences, and solutions,” she said. By using stunning, innovative graphics and avoiding confounding technical terms, ENGAGE’s products are designed to reach non-technical policy audiences and influential decision-makers.
As one of the Uganda conference’s most talked about presentations, “Uganda on the Move” wows audiences with visuals created using Hans Rosling’s Trendalyzer software. The presentation shows that although Ugandans are increasingly healthier, have a higher life expectancy, and are more educated, maternal health remains in jeopardy. Tellingly, 46 percent of pregnancies in the country are unplanned, 6,000 women die each year from complications related to pregnancy, and 1,200 women die each year from undergoing unsafe abortions.
Maternal deaths, however, do not tell the whole story: For every one woman dying, Smith said, 20-30 women suffer from short-term disability, which places a major strain on economic growth. From 2004 to 2013, maternal death will cost Uganda US$350 million in lost productivity; and disability will cost and additional US$750 million.
What Next? The African Perspective“After 10 years of virtual clandestine work, [family planning] is just coming out of the closet,” said Sahlu Haile. Over the last few decades, family planning advocates have been struggling to: 1) keep family planning alive—without it being affected by political considerations 2) make family planning a health priority, without any associations with rights violations; and 3) be in solidarity with pioneering organizations of the family planning movement, like the International Planned Parenthood Federation, that were victims of discriminatory funding decisions.
The Uganda conference changed all that, said Haile. In Uganda, conference attendees were “talking about family planning…not reproductive health, not maternal/child health.” This, he said, was “probably the single most important lesson…that I took from the Kampala conference.”
Following the conference, Haile said that African government officials stressed family planning as a priority at meetings in Ethiopia and Nigeria—the first time he had witnessed such high-level attention to family planning from those countries in his 30-year career.
In Ethiopia, African leaders pledged to:- Prioritize family planning, since family planning is one of the most cost-effective development investments;
- Ensure access to contraception, as 40 percent of maternal deaths are associated with unwanted pregnancies; and
- Integrate MDG 5b, universal access to reproductive health, into their international development plans and budgets.
Haile credited the Kampala conference for spurring these efforts. In December, he joined a task force of 14 Ethiopian organizations to plan the next steps. They will jointly develop research capacities, generate evidence, and strengthen monitoring and evaluation practices, especially with regard to integrating population, health, and environment efforts. In addition, they will engage with wider audiences via new tools such as the blog RH RealityCheck and Gapminder Foundation’s Trendalyzer program.
Haile believes we need to “work together to encourage national-level efforts…to make sure family planning stays where it is now and make sure it is not abandoned.”
To be a part of the new online family planning community, join the Kampala Conversation.
Photo 1: A women and her children in Jinja, Uganda. Courtesy Flickr user cyclopsr. Photos of Amy Tsui, Rhonda Smith, and Sahlu Haile courtesy of Dave Hawxhurst, Woodrow Wilson Center. -
‘Wilson Center on the Hill:’ Haiti’s Long Road Ahead
›March 25, 2010 // By Wilson Center StaffNearly two months after the devastating 7.0 magnitude earthquake in Port-au Prince, Haiti, the country still needs assistance to provide basic healthcare and shelter, in addition to rebuilding Haiti’s economy, government, and institutions. As the international community and NGOs make the transition from emergency disaster relief to long-term reconstruction and capacity-building efforts, donor coordination and long-term commitment are crucial. Recently, on Capitol Hill, a panel of experts organized by Wilson Center on the Hill and the Wilson Center’s Latin American Program discussed Haiti’s continuing problems and challenges.
Patience Necessary
Johanna Mendelson Forman, a senior associate for the Americas Program at the Center for Strategic and International Studies, stressed that progress in Haiti will take time—perhaps five years to rebuild and 10 years to see positive economic growth. This timeline is often frustrating for donors—including Congress and U.S. citizens—who want to see immediate results, she noted. Nevertheless, Mendelson Forman discounted the myth that “because Haiti is a weak state it is not a sovereign state,” and emphasized that developing and strengthening the Haitian government remains necessary.
She observed that the post-earthquake efforts in Haiti have been different from previous United Nations interventions, particularly in terms of the Latin American community’s involvement. Brazil, for example, is leading relief operations. Other Latin American countries—including Haiti’s neighbor, the Dominican Republic—have committed to promoting a stable and secure Haiti. Here Mendelson Forman noted a new partnership initiated by the Dominican and Haitian governments. “[Dominican officials] understand that they are doomed if Haiti is doomed,” she said. “As members of the international community, it is our job to foster that reconciliation.”
Costs Are Rising
Andrew Philip Powell, a regional economic advisor in the Caribbean Country Department at the Inter-American Development Bank (IDB), said that while the IDB initially estimated damage from the earthquake at about $8 billion, the complete destruction of the government and commerce centered in Port-au-Prince could push that number much higher. The IDB and partner organizations are currently conducting a Post-Disaster Needs Assessment that will ultimately identify the official damages and ballpark the cost of reconstruction.
Powell stated that Haiti is “not starting from a blank slate,” citing a development strategy agreed upon in April 2009 by the Haitian government and international donors. In keeping with the strategy, he emphasized the need for effective coordination between donors and the Haitian government. At the same time, he said it is vital to encourage population dispersion by shifting government agencies and private-sector jobs to other parts of the country. Haiti needs roads and communication networks outside of the capital area, as well as export processing zones in outlying regions, to increase the economic opportunities outside of Port-au-Prince, he said.
However, with the large amounts of aid flowing into the country, Powell warned donors and Haitian officials to remain on the lookout for “Dutch disease”—a decline in the manufacturing sector following a sharp increase in natural resource prices, foreign assistance, or foreign direct investment. Its occurrence could increase Haiti’s dependency on aid in the future.
Challenges for Healthcare
Sheri Fink, a public policy scholar at the Woodrow Wilson Center and senior fellow at the Harvard Humanitarian Initiative, offered her perspective on Haiti’s continuing health crisis based on two trips to the country in the earthquake’s aftermath. There are signs of hope, including some normalcy and commerce returning to the camps, she noted, but problems in the health sector as a whole are increasing. As field hospitals put in place after the earthquake close, “there is a fear among Haitians that attention is starting to turn elsewhere,” she said.
According to Fink, “the work is far from done” in Haiti, a sentiment she said is shared by many departing health workers. The hospitals left standing are not prepared to deal with the influx of patients arriving at their doors following the closure of field hospitals, and government health workers are currently working without pay.
Fink also pointed out the risk of long-term earthquake-related health problems, including injuries suffered during aftershocks or from falling debris, inflamed chronic diseases, horrible conditions and lack of basic health services in camps, and the “looming nightmare” of infectious disease epidemics.
Fink called for more international involvement to avert a widening of the health crisis. “We’ve made a big commitment and to follow-up on the investment, to make it mean something; let’s not be satisfied with just bringing things back to where they were,” she said.
By Sarah Huston and David Klaus of Wilson Center on the Hill at the Woodrow Wilson International Center for Scholars.
Photo: Courtesy Flickr user United Nations Development Programme -
The Feed for Fresh News on Population
›March 25, 2010 // By Wilson Center StaffUSAID’s Gloria Steele offers written testimony on the FY2011 Global Health and Child Survival (GH CS) budget request before the House Appropriations Subcommittee on State, Foreign Operations
Andrew Revkin gives a shout-out to family planning and notes the lack of population discussion at Copenhagen in his blog post, “From Wishful Thinking to Real-World Action on Climate“
Video of Secretary of State Hilary Clinton addressing the Commission on the Status of Women in which she discusses the Global Health Initiative, maternal mortality, family planning, and “gendercide“
Family planning-environmental connections headline PATH‘s March edition of Outlook
Youth bulges and social conflict are noted in Nicholas Kristoff’s recent article on child marriages in Yemen
Follow Geoff Dabelko on Twitter for more population, health, environment, and security updates -
Maternal and Newborn Health as a Priority for Strengthening Health Systems
›Among the many initiatives that have recently been launched to strengthen health systems in the developing world, there is little consensus on execution. Traditional strategies for improving the health system, such as the vertical approach, which prioritizes communicable diseases, or the horizontal approach, which prioritizes non-communicable diseases, are limited in scope and fail to include a comprehensive gender lens.
To overcome the shortcomings of these two health financing approaches, the “diagonal” strategy combines them by “clearly defining priorities and utilizing these priorities to drive general improvements of the health system,” said Julio Frenk, dean of the Harvard University School of Public Health, at the Global Health Initiative’s third event in the “Advancing Policy Dialogue on Maternal Health” series.
Along with panelists Helen de Pinho of Columbia University, and Agnes Soucat of the World Bank, Frenk discussed how prioritizing key maternal health indicators can improve health systems and support the implementation of evidence-based interventions.Putting Women and Health First
Drawing on his experience as Mexico’s minister of health, Frenk said that clearly defining a set of priorities grounded in “women and health” drove the improvement of Mexico’s health system. “Picture three concentric circles. The core of these concentric circles is the prevention of maternal mortality and disability; the second circle [includes] other aspects of sexual and reproductive health in addition to pregnancy and delivery; the third circle includes other fundamental areas of women’s health and the intersection of women with the health system,” said Frenk.
Mexico used maternal mortality rates to measure quality of care and rectify weaknesses in the health system. “Every maternal death triggered an audit that could lead to a hospital losing its license to operate,” said Frenk. Additionally, these audits helped to identify gaps and prioritize investments in “equipment and supply of drugs…and networks [for] obstetric emergencies,” he added.
“This illustrates how you can take a specific set of priorities and drive them through,” argued Frenk. “Global health needs to get out of the traditional confines that have split the community between vertical and horizontal and adopt more integrated frameworks like the notion of women and health,” he said, which “will leave behind a better health system to deal with the next challenge.”
Measuring Maternal Health
The maternal health community agrees that to reduce maternal mortality rates, access to emergency obstetric care (EmOC) must be improved. “A simple assessment of an emergency obstetric care facility combines a number of aspects that are core to strong health systems,” said de Pinho. To reduce maternal mortality, a strong health system must be able to positively answer these key questions:
These questions monitor the availability, utilization, and quality of care, which signals whether “the health system is actually responding to the woman’s needs when they need it,” said de Pinho. These maternal health indicators “paint a picture for where next steps need to be taken,” she said.- Are there enough facilities providing EmOC and are they well distributed?
- Are women with obstetric complications using these facilities?
- Is the quality of the EmOC services adequate?
Rwanda’s Innovations in Health Financing
“When we talk to ministries of health we ask them what are the low-hanging fruits we can reach in the six years” until the deadline for meeting the Millennium Development Goals (MDGs), said Soucat. To implement methods with proven results, additional research data, monetary support, and political will are all necessary. Rwanda’s ministry of health used the health-related MDGs—particularly MDG 5 to reduce maternal deaths by 75 percent—to reform the health system and hold institutional and individual actors accountable.
Rwanda’s health system was reformed through five key pillars:
“The heart of the reform is to increase accountability to its citizens,” said Soucat. Rwanda’s results-based financing offered “incentives and salary supplements to workers who saw more patients and provided higher quality of care,” she said. Impact assessments demonstrate that all income groups in Rwanda benefited from this health care scheme; in three years family planning tripled and assisted deliveries increased by 13 percent –“something that has never been observed in Africa,” she said.- Fiscal decentralization increased community participation and allocated funds to district governments
- Performance contracts were established between the president and district mayors
- A performance-based financing system distributed money to health facilities based on results
- Community health insurance increased access and reduced out-of-pocket expenditures
- Autonomous health facilities were allowed to hire and fire personnel
Rwanda’s Ministry of Health conducted rigorous assessments to ensure quality services and demonstrate impact to the Ministry of Finance. “When talking about maternal health a strong dialogue between the Ministry of Health and Ministry of Finance is needed more than ever and centered around the production of results,” argued Soucat. Scaling up the results-based finance scheme in other African countries is possible, she said, but additional research is needed to better understand this scheme at the decentralized level. -
Family Planning and Reproductive Health
›Adding it Up: The Costs and Benefits of Investing in Family Planning and Maternal and Newborn Health, a report by the Guttmacher Institute, asserts that “sustained and increased investment in sexual and reproductive health services in developing countries” would “contribute to economic growth, societal and gender equity, and democratic governance.” The report presents cost-benefit analyses of family planning and maternal and newborn health strategies in an effort to “guide decision makers, at the global, regional and country levels, in making investments that would reap the greatest returns for individuals and societies.”The Interagency Gender Working Group recently released Gender Perspectives Improve Reproductive Health Outcomes: New Evidence, argues for the importance of taking gender into consideration when developing interventions related to unintended pregnancies, maternal health, STIs, harmful practices (e.g. early marriage, genital cutting, and gender-based violence), and youth. The report, a follow-up to 2004’s The “So What?” Report: A Look at Whether Integrating a Gender Focus into Programs Makes a Difference to Outcomes, includes 40 specific examples of programs successfully integrating gender to improve reproductive health.








 Putting Women and Health First
Putting Women and Health First


 The
The 
