Showing posts from category global health.
-
How Did We Arrive at 7 Billion – and Where Do We Go From Here? [Part Two]
›October 26, 2011 // By Elizabeth Leahy MadsenThe world’s women will determine whether the global population in 2050 is as low as 8 billion or as high as 11 billion through their choices (or lack thereof) about the number and timing of their children. Women in developing regions of the world will have the greatest effect on these potential population trajectories. Even if fertility rates remain constant at current levels (which is unlikely), developing regions would grow from 5.7 billion in 2010 to 9.7 billion in 2050, but the total population of developed countries would remain essentially unchanged. The UN estimates that the seven billionth person alive today will be born on October 31. Demographer Elizabeth Leahy Madsen explains how we got to that number, its significance, and where our demographic path might take us from here. Read part one here.
The UN estimates that the seven billionth person alive today will be born on October 31. Demographer Elizabeth Leahy Madsen explains how we got to that number, its significance, and where our demographic path might take us from here. Read part one here.
The world’s women will determine whether the global population in 2050 is as low as 8 billion or as high as 11 billion through their choices (or lack thereof) about the number and timing of their children. Women in developing regions of the world will have the greatest effect on these potential population trajectories. Even if fertility rates remain constant at current levels (which is unlikely), developing regions would grow from 5.7 billion in 2010 to 9.7 billion in 2050, but the total population of developed countries would remain essentially unchanged.
The way that people decide the timing and number of their children is not easily distilled into a simple formula with a single solution. Still, some basic and important facts are known. In the developing world, where more than 80 percent of the world’s population lives, women in rural areas, those who have little or no education, and those who are poor, have larger families. As demographers have shown in modeling the determinants of fertility, women tend to seek contraception once they are confident that their children will survive to adulthood and when socioeconomic development increases the “costs” of having children, for example by motivating parents to send them to school rather than to work.
One of the most direct reasons for past declines in fertility rates was the rapid expansion of family planning and reproductive health programs, supported by country governments and international donors, that enabled women and men to more effectively choose the size of their families. But today, about 215 million women across the developing world would like to delay or avoid pregnancy but are using ineffective contraception or none at all. Funding programs to meet the family planning needs of these women, which would cost about $3.6 billion annually, would both empower them and help fertility rates continue to decline.
Beyond Access: Gender Inequality Inhibits Contraceptive Use
While increasing support for family planning programs tops the list of demographers’ recommended policies, ensuring that contraceptives are available and accessible will not alone achieve the fertility declines projected in most of the UN’s range of possibilities. Many women who are having or planning to have large families know about family planning and where to find it, but are choosing not to use contraception for cultural reasons that are often deeply engrained.
In sub-Saharan Africa, the region with the highest global fertility rate, only 16 percent of married/partnered women of reproductive age are using effective contraception. In comparison, between 62 and 75 percent of their peers in Ireland, the United States, and Uruguay – countries whose fertility rates are almost exactly at replacement level – are using it.
Logically, sub-Saharan Africa needs similar levels of contraceptive use to bring its average fertility rate towards replacement level as the UN projects, so the region’s average prevalence rate for modern contraception would need to rise by at least 10 percentage points in each of the next four decades. However, contraceptive use in the region has grown by only 0.5 percentage points or less over the past 30 years.
What is inhibiting the use of contraception? Demographic and health surveys find in Nigeria, for example, that 10 percent of married women are using an effective contraceptive method, while twice as many have an unmet need for family planning. This low use of family planning demonstrates high potential for change in the country’s demographic future, which, as the most populous in Africa, will greatly influence global and regional trends. Yet among women who do not intend to use contraception, 39 percent report that they or their family members are opposed to family planning, and another 16 percent fear side effects or have other health-related concerns. If Nigeria’s fertility rate remains unchanged, the country will be home to 500 million people by 2050.
In Pakistan, where 24 percent of births are unintended, surveys show similar barriers. Ninety-six percent of married women know about effective contraceptive methods, but only 22 percent are using one. More than one-quarter of women who do not plan to use contraceptives report that their fertility is “up to God” and 23 percent report that they or their family members are opposed to family planning. Pakistan’s population would more than double from 174 million to 379 million by 2050 if current fertility trends hold constant.
Peak Planet? Population Growth and Consumption Strain Environmental Resources
Because Nigeria, Pakistan, and other countries’ demographic trajectories may not follow the path laid out in population projections, we can’t take a world of nine billion for granted. While human ingenuity and technological advancements have improved standards of living in many countries, scientists caution that the combination of rising human numbers and growing consumption has serious environmental implications. Already, the quantity and quality of fresh water supplies are under strain, and forests in many developing countries are being rapidly depleted.
Population projections are much more than wonkish speculation – they foreshadow the serious problems that lie ahead if health, environment, and development policies aren’t strengthened. If the UN projections of our demographic future are to bear any semblance of reality, we must move beyond the status quo. While improving physical access to family planning should remain a top priority, meeting unmet need will also require addressing the deep-seated challenges of women’s education and empowerment.
Elizabeth Leahy Madsen is a consultant on political demography for the Wilson Center’s Environmental Change and Security Program and former senior research associate at Population Action International.
Sources: Bongaarts and Sinding (2009), Bongaarts (2006), Futures Institute, Guttmacher Institute and UN Population Fund, Measure DHS, O’Neill, Dalton, Fuchs, Jiang, Shonali Pachauri, and Katarina Zigova (2010), UN Population Division, Washington Post.
Photo Credit: “Afghan Internally Displaced Persons,” courtesy of flickr user United Nations Photo. -
Carl Haub, Behind the Numbers
Rwanda’s 2010 Demographic and Health Survey Shows Remarkable Drop in Fertility and Child Mortality
›October 18, 2011 // By Wilson Center StaffThe original version of this article, by Carl Haub, appeared on PRB’s Behind the Numbers blog.
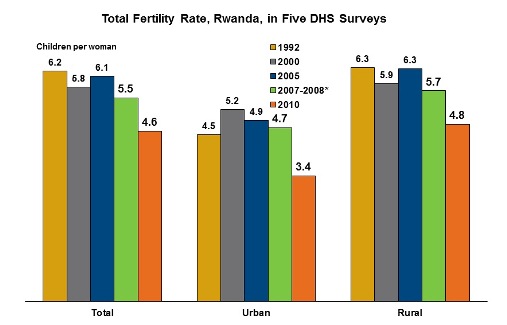
The Rwanda 2010 Demographic Health Survey is the latest in a regular series of DHS surveys that began in 1992, although hostilities had delayed the next survey until 2000. The 2010 survey interviewed 13,671 women ages 15 to 49 and 6,329 men ages 15 to 59 from September 2010 to March 2011. The total fertility rate (TFR – the average number of children would bear in her lifetime if the birth rate of a particular year were to remain constant) obtained in the survey was 4.6 for the three-year period preceding the survey. For urban women, the TFR was 3.4 and for rural women, who were 85 percent of the sample, 4.8.
Rwanda’s TFR saw its fastest decline in the 2010 DHS. From the 2007-08 Interim DHS to the 2010 survey, the TFR fell by 1.1 children nationwide – by 1.3 in urban areas and 0.9 in rural areas in a period of only four and a half years. This is sharpest drop in a sub-Saharan TFR I can ever remember seeing. As an indicator of future fertility plans, 56.2 percent of women with three living children said that they not wish to have any more children as did 76 percent of those with four living children. It is clear that the large family size of eight children per woman is truly a thing of the past.
In the survey, 51.5 percent of currently married women said that they were using some form of family planning, 45.1 percent a modern method. Injectables were by far the most frequently used, as such “spacing” methods are in much of Africa, with 23.1 percent of women saying that they used them. That method increased from 15.2 percent in the 2007-08 survey. The next two methods were implants (6.3 percent) and the pill (7.1 percent).
Continue reading on Behind the Numbers.
Image Credit: Arranged by Population Reference Bureau; data from the National Institute of Statistics of Rwanda, Ministry of Finance and Economic Planning, Ministry of Health Rwanda, MEASURE DHS, ICF Macro, Demographic and Health Survey 2010, Preliminary Report. -
Lisa Hymas on Envisioning a Different Future With Family Planning in Ethiopia
›ECSP caught up with Lisa Hymas, senior editor at Grist, last week during the first South by Southwest (SXSW) Eco conference and she spoke about her recent visit to Ethiopia to see the country’s community health extension program in action. “Ethiopia has a big challenge around population,” Hymas said, “but the government is committed to bringing that down.”
The government extension program places health-workers – young women, for the most part, who have received basic training – directly into each community, where they are able to give out immunizations, provide advice on nutrition, teach families how to properly hang bed nets to prevent mosquito-borne illnesses, and provide family planning services and advice.
Thanks to the program, these health workers and those in the communities they service can “envision very different lives for themselves than their mothers had,” Hymas explained. For instance, one woman recounted that her mother gave birth to 10 children, “and almost died giving birth to the last one, because there was no access to birth control, and there was no good access to health care.” In contrast, she is now able to have a career and to use family planning to delay and space her own childbearing.
For more on Ethiopia’s health extension program, see Schuyler Null’s report on visiting a village health clinic near the town of Fiche last spring. -
Silent Suffering: Maternal Morbidities in Developing Countries
›Maternal morbidities – illnesses and injuries that do not kill but nevertheless seriously affect a woman’s health – are a critical, yet frequently neglected, dimension of safe motherhood. For every woman who dies, many more are affected acutely or chronically by morbidities, said Karen Hardee, president of Hardee Associates at the Global Health Initiative’s September 27 panel discussion, “Silent Suffering: Maternal Morbidities in Developing Countries.” Hardee was joined by Karen Beattie, project director for fistula care at EngenderHealth, and Marge Koblinsky, senior technical advisor at John Snow, Inc., for a discussion moderated by Ann Blanc, director of EngenderHealth’s Maternal Health Task Force.
-
Ben Ramalingam, Aid on the Edge of Chaos
The Complexity of Scaling Up
›October 11, 2011 // By Wilson Center StaffThe original version of this article, by Ben Ramalingam, appeared on Aid on the Edge of Chaos.
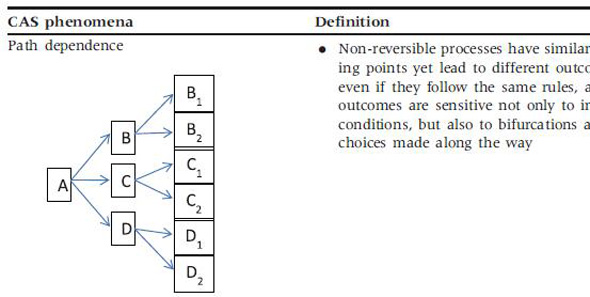
Despite increased prominence and funding of global health initiatives, attempts to scale up health services in developing countries are failing, with serious implications for achieving the Millennium Development Goals. A new paper argues that a key first step is to get a more realistic understanding of health systems, using the lens of complex adaptive systems.
Much ongoing work in development and humanitarian aid is based on the idea of “scaling up” effective solutions. Healthcare is one of the areas where this idea has played a central role – from the World Health Organization’s Health for All in the 1960s to UNICEF’s child healthcare programs, from rolling out HIV-AIDS, malaria and TB treatments to the package of interventions delivered to achieve the Millennium Development Goal on health.
However, despite the fact there are many cost-effective solutions to health problems faced in developing countries, many agencies are still frustrated in their attempts to deliver them at scale. This may be because of a widespread failure to understand the nature of health systems.
Continue reading on Aid on the Edge of Chaos.
Image Credit: Adapted from Table 1, “Understanding pathways for scaling up health services through the lens of complex adaptive systems,” Health Policy and Planning, Oxford University Press. -
SXSW Eco Panel: Three Great Ideas That Won’t Be On the Rio+20 Agenda
›September 30, 2011 // By Schuyler NullSouth by Southwest (SXSW) – the popular music, film, and alternative showcase – is moving into the green space with its first ever “eco” conference, kicking off next week, October 4, with more than 50 panels on “solutions for a sustainable world.” There’s one in particular though you should tune into: “Three Great Ideas that Won’t Be On the Rio Agenda,” featuring Geoff Dabelko, director of the Wilson Center’s Environmental Change and Security Program; Roger-Mark De Souza, vice president of research and director of the climate program at Population Action International; and Aimee Christensen, CEO of Christensen Global Strategies.
The panel will feature discussion on three issues that will likely not be on the table at the Rio+20 UN Conference on Sustainable Development next year: integrated population, health, and environment development programs, climate adaptation as a path to peacebuilding, and how to get the private sector better involved in helping cope with climate change.
If you’re traveling down to Austin, “Three Great Ideas” is scheduled for Thursday, October 6 at 10am CST; if not, stay tuned for webcast information! -
Women Leaders Urge Stronger Advocacy on Health and Public Policy
›The original version of this article appeared on the Pan American Health Organization website.
Women have made major strides toward greater equality in Latin America and the Caribbean, but stronger advocacy and leadership are needed to address problems they continue to face in health and other areas, said a group of top women health leaders at an event held at the Woodrow Wilson Center in Washington, D.C. on September 27.
The event was part of a series of activities surrounding the 51st Directing Council meeting of the Pan American Health Organization/World Health Organization (PAHO/WHO), which is being held this week.
Dr. Michelle Bachelet, Executive Director of UN Women, noted that Millennium Development Goal (MDG) five, reduce maternal mortality, “is the one MDG that has advanced the least in our region and around the world.” She said it is now widely accepted that investing in women is not only an issue of human rights, it is also “the intelligent thing to do economically, politically, and socially. So why doesn’t it happen?” She said making it happen is the major leadership challenge facing women in health and public policy today. “We have to empower women to make the strongest case possible that investing in women is the best thing governments can do, and we have to help ministers of health make this same case with their governments.”
WHO Director-General Dr. Margaret Chan said that high levels of maternal mortality reflect “a failure of governments.” “We know how to prevent women from dying while giving birth. It’s a lack of political commitment, policies, and investments in the right areas. We need to get these issues out into the public, and we need to work with men who are enlightened to accomplish this,” she said.
Rocío García Gaytán, President of the Inter-American Commission of Women, said maternal mortality continues to be a major problem in the hemisphere despite the fact that it is almost completely preventable. She said that contrary to common belief, most maternal deaths take place in hospitals and are the result of a lack of proper training of medical personnel. “This problem should not exist in the second decade of this millennium,” she said.
PAHO Director Dr. Mirta Roses urged women to develop a leadership style that will effectively advocate for women’s top concerns, particularly social, economic, and political progress.
“What is different when women lead?” Roses asked. “We need to support each other and identify what we should do that is different from male models. We must all work together – UN Women, the Council of Women World Leaders – to define feminine leadership and promote it.”
Canada’s Minister of International Cooperation, Beverly Oda, said progress on public policies for women “took many years” to develop in Canada. Today, gender reviews of legislation are now mandatory for legislation, and promotion of gender equality is an integral part of Canadian technical cooperation programs.
Vice-Minister of Health Dr. Silva Palma de Ruiz of Guatemala described a number of initiatives in her country that have been successful in improving women’s health and status. They include joint efforts involving the health ministry, the public prosecutor’s office, the national human rights ombudsman, and civil society organizations to reduce sexual violence by empowering women to report violence and by more aggressive prosecution of perpetrators. PAHO/WHO has supported these efforts with technical assistance in developing guides for care of victims of sexual violence. Other efforts include a new family planning law and education of men and women as well as healthcare workers about women’s rights to use contraception.
Minister of Health Ann Peters of Grenada said that women of the Caribbean “are very vocal” and have had considerable success advocating for women’s health. In her own country, this has helped produce a highly effective comprehensive mother-child health program that includes strong community health services with well-trained midwives and good referral systems, breastfeeding-friendly hospitals, and universal voluntary testing of pregnant women for HIV. Thanks to these programs, Grenada has “no mother-to-child transmission of HIV and virtually no maternal mortality.”
Minister of Health Marcella Liburd of Saint Kitts and Nevis noted the importance of addressing the social determinants of women’s health. For example, in her country as elsewhere, the majority of people living in poverty are women. “We need to consider other aspects of women’s well-being,” she said, “including financial, social, and mental health.”
Paraguay’s Minister of Health, Dr. Esperanza Martinez, said it was important to address women’s concerns in an integral way. She described a new platform for discussing policies that affect women involving different government ministries, not just health. “Women need to participate as policymakers and also to influence policies from the outside,” she said.
Dr. Carmen Barroso, Western Hemisphere Director for the International Planned Parenthood Federation, said, “Civil society is ready to partner with ministries of health to advocate for more resources, legislation, and promotion of women’s sexual and reproductive rights.”
The event was organized by the Council on Women World Leaders, PAHO/WHO, the Wilson Center’s Environmental Change and Security Program, Global Health Initiative, and Latin America Program.
Event ResourcesPhoto Credit: David Hawxhurst/Wilson Center. -
Carl Haub, Behind the Numbers
Ethiopia’s 2011 Demographic and Health Survey: Remarkable Fertility Decline, Continued Rural Health Challenges
›September 28, 2011 // By Wilson Center StaffThe original version of this article, by Carl Haub, appeared on the Population Reference Bureau’s Behind the Numbers blog.
Continuing my recent practice of posting a quick summary of results from new demographic surveys in developing countries, here is another new Demographic and Health Survey (DHS) preliminary report, this time from a sub-Saharan African country. This will help readers of this blog to stay right up-to-date with the latest developments.
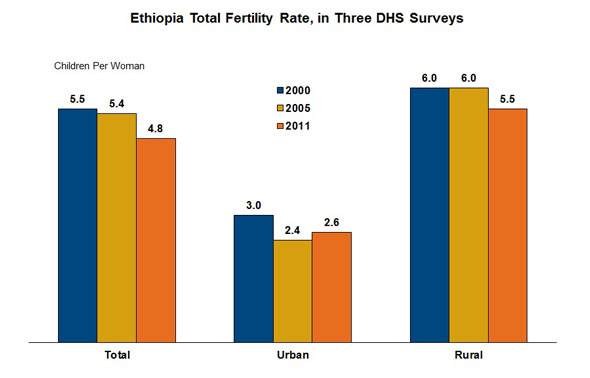
The Ethiopia 2011 DHS interviewed 16,515 women ages 15 to 49 and 14,110 men ages 15 to 59 from September 2010 to June 2011. The total fertility rate (TFR – the average number of children would bear in her lifetime if the birth rate of a particular year were to remain constant) obtained in the survey was 4.8 for the three-year period preceding the survey. For urban women, the TFR was 2.6 and for rural women, who were a little over 75 percent of the sample, 5.5. There appears to have been an acceleration of TFR decline from the 2005 to the 2011 survey compared with the 2000 DHS, which had a three-year TFR of 5.5. In 1990, a government survey had shown the TFR as 6.4. The desire to continue or cease childbearing provides one insight into possible future fertility trends. Of the women with five living children, 55.8 percent said that they did not wish to have any more children; among women with six or more living children, 68.6 percent said that they also wished to ceased childbearing.
Continue reading on Behind the Numbers.
Image Credit: Population Reference Bureau; data courtesy of Ethiopian Central Statistics Agency (CSA) and ICF Macro, Ethiopia Demographic and Health Survey (EDHS) 2011, Preliminary Report.