Showing posts from category global health.
-
Eliya Zulu on Population Growth, Family Planning, and Urbanization in Africa
› “The whole push for population control or to stabilize populations in Africa in the ’70s and the ’80s mostly came out of the West,” said Eliya Zulu of the African Institute for Development Policy (AFIDEP) in this interview with ECSP. Then new research brought to light the fact that many women in Africa actually wanted to control their fertility themselves, but they didn’t have access to family planning.
“The whole push for population control or to stabilize populations in Africa in the ’70s and the ’80s mostly came out of the West,” said Eliya Zulu of the African Institute for Development Policy (AFIDEP) in this interview with ECSP. Then new research brought to light the fact that many women in Africa actually wanted to control their fertility themselves, but they didn’t have access to family planning.
“It kind of put the African leaders who really didn’t want to talk anything about fertility control and so on in a fix,” Zulu said. “Because all of sudden now it was the African women themselves who are saying we need these services – it was not an imposition from the West.”
Based in Nairobi, Kenya, Zulu said that part of what he does at AFIDEP is “try to get African countries to think about the future.” Current economic growth in parts of Africa simply can’t match population growth, but improving access to family planning and child/maternal health infrastructure can greatly reduce fertility rates – and quickly.
“The question for Africa is: Are we going to be ready? And we need to prepare,” said Zulu. “For that to happen it’s not just about saying ‘let’s have fewer children.’ I think we also need to do this from a social developmental perspective where we also look at ways in which we can improve the quality of the population, empower women, invest in education, and so on.”
Four Factors of Success
There are several factors that are critical for successful family planning and child/maternal health efforts, said Zulu: strong political leadership, sustained commitment over time, financial investment (research has shown that over 90 percent of women in sub-Saharan Africa cannot afford contraceptives), and strong accountability mechanisms for monitoring performance of programs and use of resources.
“There are a number of countries that have shown that, even with the limited resources that Africa has, that with all the problems that Africa has, if you really emphasize those four factors that I mentioned, you can actually achieve very, very positive results,” Zulu said.
Rapid Urbanization and the Growth of Urban Poverty
Rapid urbanization is one of Africa’s biggest challenges, said Zulu. “Africa is the least urbanized region of the world now, but it’s growing at the highest rate.” If you look at historical examples from the West and Asia, “urbanization is supposed to be a good thing; urbanization has been a driver of economic development,” he said, but “the major characteristic of urbanization in Africa has been the rapid growth of urban poverty.”
“If the economies are not going to develop the capacity to absorb this population and create enough jobs for them, there’s going to be chaos, because you can’t have all these young people without having jobs for them,” said Zulu. “The challenge for many African governments is how to have sustainable urbanization and how to transform our cities into agents of development.”
The “Pop Audio” series is also available as podcasts on iTunes. -
Reality Check: Challenges and Innovations in Addressing Postpartum Hemorrhage
›Heavy bleeding after childbirth, also known as postpartum hemorrhage (PPH), is one of the leading causes of maternal deaths worldwide. Globally, approximately 25 percent of all maternal deaths are caused by postpartum hemorrhage, and many mothers bleed to death due to delays in seeking health care services. On January 25th, 100 representatives from the maternal health community – a majority working directly in developing countries – convened for an all-day meeting at the Wilson Center to discuss experiences in the field and perform “reality checks” on the challenges and successes of PPH programs.
-
Albert Lotana Lokasola, PHE Champion
Improving Health and Preserving Ecosystems in the Democratic Republic of Congo
›This PHE Champion profile was produced by the BALANCED Project.
In the remote forests of the Democratic Republic of Congo (DRC), Albert Lotana Lokasola is helping improve livelihoods by bringing much-needed health services to the communities living in and around the Kokolopori Bonobo Reserve. Officially recognized by the DRC government in May 2009, the reserve is a high biodiversity wilderness area covering an area about the size of Rhode Island (4,785 square kilometers).
Located 300 miles southwest of Kisangani, the reserve contains bonobos, a rare and highly endangered great ape species that is as closely related to humans as chimpanzees. In addition, the reserve is highly valued for its biodiversity, including several other flagship species such as leopards, elephants, Congo peafowl, Tshuapa red colobus, and Salonga monkeys.
Lokasola founded a nationally recognized organization called Vie Sauvage, or “Wild Life” in English. He serves as the president of the organization and works with international organizations to foster conservation and rural development in an integrated, holistic approach. As a native of Kokolopori, he believes that “the forest, men, and wildlife live together and should be protected together.”
In partnership with local residents and supported by the Bonobo Conservation Initiative, Lokasola and Vie Sauvage established the first medical clinic in the area in 2006. They garnered support for a doctor, nurses, and supplies from the Indigo Foundation in Australia and the Kokolopori-Falls Church Sister City Partnership.
Before the clinic was founded, community members had to walk or bicycle more than 50 miles to get to the nearest hospital in the territorial capital of Djolu. Now the Kokolopori clinic serves the 8,000 people who live in 30 villages along a 40-mile road in the reserve. One of the clinic’s goals is to help improve women’s health by training and equipping midwives and by providing access to other health services. Malaria and poor nutrition contribute to high maternal and child mortality, and women in Kokolopori do not yet have access to reproductive health services such as family planning.
Vie Sauvage articulates integrated health and conservation messages through their community education projects. They are also working with the community to prevent malnutrition by planting fruit trees in agroforestry fields to produce supplemental food supplies. At the same time, these trees will create corridors for wildlife movement and protect the genetic flow. They also create a sound micro-climate for people, sequester carbon dioxide, and filter the air. Through these efforts, Vie Sauvage and the people of Kokolopori are demonstrating the critical links between human well-being and conservation.
Vie Sauvage has garnered resources and participation from diverse partners (like the Kokolopori-Falls Church Sister City Partnership and the Indigo Foundation, mentioned above) which work together to support the clinic and fund medical staff salaries, training, supplies and equipment, and infrastructure improvements.
According to Lokasola, Vie Sauvage and partners are currently exploring potential partnership opportunities to integrate family planning and reproductive health into existing activities. His hope is that by providing these much-needed services, the community will be healthier and critical ecosystems will be sustainably preserved.
This PHE Champion profile was produced by the BALANCED Project. A PDF version can be downloaded from the PHE Toolkit. PHE Champion profiles highlight people working on the ground to improve health and conservation in areas where biodiversity is critically endangered.
Photo Credit: Building along the road in Kokolopuri village serves as a messsage drum for sending messages from one village to the next, courtesy of Ingrid Schulze and the BALANCED Project. -
ASRI’s Integrated Health and Conservation Programming in Borneo
›If you have a fever in the town of Sukadana in Indonesian Borneo, the locals might suggest you go to the ASRI clinic. It’s in a little house whose front yard is crowded with bicycles and motorbikes. In the waiting room, you examine a whiteboard that explains your payment options. ASRI accepts cash. But it looks like you can also pay with labor in the clinic’s organic garden or its reforestation site. If you own a goat, you can bring in its manure and pay with that. You can even pay with durian tree seeds!
Doctoring both humans and the environment is the raison d’etre of Alam Sehat Lestari (“healthy life everlasting” in Bahasa Indonesia, or ASRI for short), an NGO dedicated to the idea that human health is so intertwined with that of the environment that trying to fix one must include trying to fix the other. Located beside Indonesia’s Gunung Palung National Park, ASRI aims to protect the park’s irreplaceable rainforests by offering health care incentives to local people to stop illegal logging. We’re supported by our sister NGO in the United States, Health in Harmony.
For both people and the forest, the task is urgent. The island of Borneo was once famously covered by rainforest. But now only half of that canopy exists, and less than one-third will remain by 2020. Beginning in the mid-20th century, loggers, palm-oil plantation companies, and farmers logged, burned, and clear-cut their way through the island. Horrifyingly, much of this destruction has taken place in “protected” areas like national parks. The relentless loss of forest has devastated biodiversity in Borneo and severely reduced habitats for many organisms, including one of humanity’s closest relatives, the orangutan – as of 2005, there were about 55,000 left, a tenth of which live in Gunung Palung. Some experts predict the orangutan will be extinct within a few decades. Despite their protected status, Gunung Palung’s forests are continually threatened by illegal logging for valuable hardwood, poor implementation of management practices, and forest fires, many of which are started to clear land for new uses. Over 50,000 hectares of the 90,000-hectare national park’s forest cover are damaged or gone.Contributing is the fact that Borneo’s economy is based largely on extractive industries; there simply aren’t many other job options. An ASRI survey found that in the Gunung Palung area the average cost of an emergency visit to the district or regional hospital was $460 – more than the average annual income. In fact, one-third of interviewees had faced a choice between health care and food. Financial pressures like that are what drive people to illegal logging. A four-meter board can go for R110,000, or about $10 – a little less than the average villager’s monthly income of $13. Working in a rice field, by contrast, pays about a dollar a day.
Sukadana, located so close to Gunung Palung, is a boom town for these industries. It was recently made a seat of the local regency. We watch new buildings go up every week – most of them built using illegal wood chopped straight out of the national park – and workers and money are flowing in.
As forest is converted to plantations, however, pesticides and fertilizers enter the watershed, which damage water and soil quality as well as human health. Watershed destruction from logging and land conversion leads to flooding which makes it harder to raise rice and can increase rates of flood-related diseases. Logging itself is dangerous work, and there are few or no worker protections. As well, seasonal, man-made forest fires, which this ecosystem is not adapted to and which can last for months, devastate both the natural habitat and respiratory health.
Enter ASRI: Our Sukadana clinic offers high-quality, low-cost medical care to all comers, with discounts for people living in villages that do not contribute to illegal logging (which the National Park office determines using air and ground patrols). This incentive system was devised in consultation with local leaders and is intended to take advantage of powerful social ties in this rural area. But given the complexity of the connections between poverty, health, and the environmental degradation here, ASRI also attacks these problems from other angles.
For one, patients and families can pay by eco-friendly, non-cash means – some of which actually end up providing further benefit to the patients. Many choose to do a stint of labor for ASRI in our organic garden. There they learn techniques that they can apply to their own crops. Some farmers have reported making a considerable profit selling their own organic produce with the skills they learned at ASRI, and some have sworn off traditional slash-and-burn agriculture, because as organic farmers they earn more money for less work. Others decide to work at ASRI’s reforestation site, which aims to restore several hectares of burned-over, degraded grassland to its original forested state. Patients can also bring in compost or manure; rainforest seeds and seedlings; or handmade grass mats, which are snapped up by clinic staff and volunteers.
ASRI’s other programs include Goats for Widows, in which impoverished widows receive a goat and give back its organic manure and one kid. Clinic staff teach townspeople and villagers about the links between the environment and health and include information about diseases like tuberculosis during “movie nights,” when they set up a projection screen and show educational videos. Crucially, ASRI also engages in capacity-building through its trained medical volunteers, who serve as consultants for Indonesian staff doctors who are fresh out of medical school.
On the horizon is a new eco-friendly “super-clinic” that will allow us to perform major surgery and house many more inpatients. We hope that as it goes up, people will learn ways to build with less wood, and that by offering even better health care to people living around the national park, we will gain enough leverage to slow or even stop illegal logging. For the community – everyone from the next generation of Sukadanans to the gibbons and durian trees – that would be a healthy change for all.
Jenny Blair, M.D., is a physician, writer, and long-term volunteer at ASRI, along with her husband, Roberto Cipriano, a LEED-accredited professional and architect who is helping to design ASRI’s newest clinic.
Sources: Center for International Forestry Research, Food and Agriculture Organization, Gunung Palung Orangutan Conservation Program, Mongabay.com, Rainforest Action Network, Tropics, World Rainforest Movement, World Wildlife Foundation
Video and Image Credit: “Conservation – Part 1,” courtesy of AlamSehatLestari, and “Ibu Nurdiah,” used with permission, courtesy of Roberto Cipriano. -
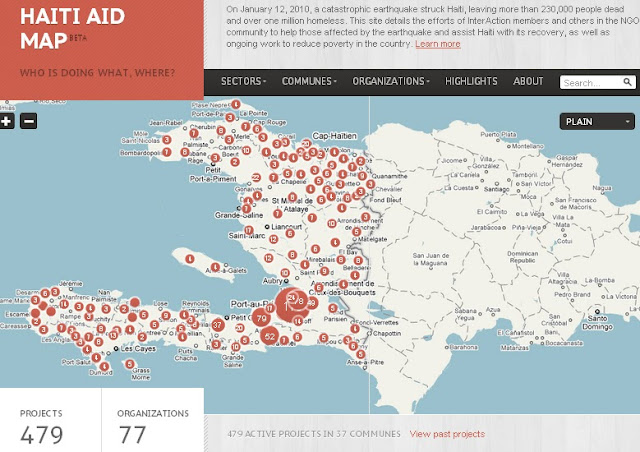
Mapping the “Republic of NGOs” in Haiti
›One year after the devastating earthquake that hit Haiti, InterAction has teamed up with the U.S. Chamber of Commerce’s Business Civic Leadership Center and FedEx to launch the Haiti Aid Map, an interactive visual mapping platform of individual aid projects being conducted in Haiti. The goals of the map are to increase aid transparency, facilitate partnerships, and help NGOs and others better coordinate and allocate resources to aid relief and reconstruction efforts.
With an estimated 10,000 NGOs operating on the ground – the second largest per capita in the world – Haiti has been referred to as “a republic of NGOs.” The Haiti Aid Map is an effort to help the humanitarian community – which has been criticized for lack of accountability, poor transparency, and corruption – better coordinate its response.
The map features 479 projects being operated all over the country by 77 local and international NGOs, most of which are InterAction members. Projects can be browsed by location, sector, or organization and include information on project donors, budgets, timelines, and the number of people reached by the project.While InterAction’s map covers their donors’ response, it leaves out the thousands of government and other NGO projects being conducted in Haiti. USAID recently released a map of U.S. government projects in Haiti (see right) by sector and location.
“The goal is not to rebuild Haiti but to build a different Haiti,” said Sam Worthington, President and CEO of InterAction, speaking exactly one year after the earthquake struck at the map’s formal launch this month. “The relief effort will still be here a year from now.” The goal of the map will be to help coordinate activities as reconstruction continues in the future.
The map is the first part of a larger mapping platform, called the NGO Aid Map, which will include not only the Haiti aid map but also projects working on food security in other developing countries. The food security map is due to be launched in March 2011.
Sources: Clinton Foundation, InterAction, NPR, ReliefWeb, USIP.
Image Credit: Adapted from Haiti Aid Map. -
Watch: Amy Webb Girard on Integrated Development Strategies for Improved Women’s Nutrition
›“When women become pregnant…their nutrient needs shoot through the roof,” said Amy Webb Girard of Emory University’s School of Public Health in this interview with ECSP and the Global Health Initiative. Girard explains that under-nutrition is a major problem for women – especially pregnant women – in resource-poor settings.
“For example, iron requirements almost double during the course of pregnancy, but iron is one of those nutrients that are really difficult to get,” Girard explained. Meat is not readily available in many developing countries and the iron in non-meat foods is not absorbed as completely. As a result, “women by and large are unable to meet those nutrient needs,” she said.
Fortunately, there is “an arsenal of nutritional interventions available,” noted Girard, including micro-nutrient supplements, behavior change strategies, and integrated facility- and community-based delivery methods.
“Additionally I think it’s very important that we also look at food production. This is a key, key thing,” said Girard. “Women who are able to produce their own foods [and] households that can produce their own foods have greater food security.”
“A lot of these agricultural strategies serve double purposes,” Girard said. “They not only increase the available food and the quality of that food, they improve women’s livelihoods, they give them a source of income, they give them – as some studies have shown – greater ability to negotiate within their own households for how money should be spent [and] whether they should access care or not. So they actually empower women in ways beyond nutrition.” -
In FOCUS: To Get HELP, Add Livelihoods to Population, Health, and Environment
›January 20, 2011 // By Wilson Center StaffProponents of integrated development have always faced significant barriers, but with a new focus on international aid from the Obama administration, the tide may be turning. To fully harness this momentum, Gib Clarke argues in a new ECSP brief that the population-health-environment (PHE) community must solidify its research base, reach out to new partners, and push for flexible funding and programming.
In “Helping Hands: A Livelihood Approach to Population, Health, and Environment Programs,” he writes that PHE programs should also add livelihoods (i.e., ways to make a living) as a critical element. He suggests such programs adopt a new moniker: “HELP” – Health, Environment, Livelihoods, and Population.
“Helping Hands” comes at a time when the integrated approach is being touted at the highest levels:“We cannot simply confront individual preventable illnesses in isolation. The world is interconnected, and that demands an integrated approach to global health,” said President Barack Obama in May 2009, echoing what population-health-environment (PHE) practitioners have long argued: Integrated lives with integrated problems require integrated solutions. Proponents of integration face significant barriers: lack of funding, programmatic silos, and policy disinterest.
While the Administration’s newest development efforts (see, e.g., Feed the Future Initiative, Global Health Initiative, and release of the QDDR) all recognize the power of integration, the degree to which these initiatives will operate across sectors remains to be seen. Drawing on interviews with leading experts, Clarke outlines the continuing challenges to implementing more integrated PHE programs and offers four recommendations for overcoming them:
“Given the strong base of existing and recent PHE programs, the PHE community is well-positioned to work with lead partners in Obama’s Global Health Initiative, climate change adaptation efforts, food security programs, and other upcoming crosscutting work,” concludes Clarke, who is currently director of planning and development at Interfaith Community Health Center in Bellingham, Washington. For example, USAID Administrator Rajiv Shah stated that the Feed the Future program would be closely integrating its objectives with the Global Health Initiative – a potential opportunity for PHE programs that offer both health benefits and food security.- The PHE community should adopt a new name that highlights the all-important livelihood component, such as “HELP Plus.”
- PHE programs need to gather data and conduct operational research to justify the claims of the PHE field.
- The PHE community needs to “agree to disagree” on the issue of scaling up integrated programs.
- PHE programs should seek funding from a diverse array of donors.
“This increased interest in integration may also be the best opportunity for finding new funding, fostering replication, and scaling up. It is a promising moment for integrated approaches, whether we call them PHE, HELP Plus, or some other acronym,” writes Clarke.
“Helping Hands: A Livelihood Approach to Population, Health, and Environment Programs” along with previous FOCUS issues are available on ECSP’s publications page.
Image Credit: From the cover of “Helping Hands: A Livelihood Approach to Population, Health, and Environment Programs,” courtesy of the Wilson Center. -
Andrew Morton, UNEP
Haiti 2011: Looking One Year Back and Twenty Years Forward
›January 14, 2011 // By Wilson Center StaffThis piece first appeared on the website of the Haiti Regeneration Initiative – a new collaborative venture between the UN, the government of Haiti, the Earth Institute at Columbia University, Catholic Relief Services, and a wide range of other implementing partners.
In 2010, Haiti endured a year like no other. The country was struck by a devastating earthquake, a cholera epidemic, floods, violence, and political uncertainty. At the same time, Haiti witnessed heroic rescue and relief efforts and an enormous demonstration of international goodwill. Today, recovery and reconstruction are taking place, albeit at a frustratingly slow pace and not currently at the scale of existing needs.
Just as importantly, 2010 brought a renewed awareness of the need for lasting solutions and improvements in the design and delivery of international aid. During the next few days, we will look back on the tragic events of January 12th, 2010, while at the same time, we must look forward, not just one year, but 20.
A Failed Recovery in a Fragile State
Already before the earthquake, Haiti was a fragile state trapped in a slow but vicious negative spiral. A tightly interconnected trio of chronic environmental, political, and socio-economic crises has gradually ensured that Haiti has had the lowest human development indicators in the Western Hemisphere, with life-long poverty, chronic hunger, and violence. Catastrophic events, such as natural disasters, epidemics, and political violence, have simply steepened the descent. Moreover, disaster recovery efforts to date have systematically failed to bring the country back to pre-disaster levels.
In spite of this depressing analysis and forecast, we should not resign ourselves to failure. The situation can be turned around but only with great effort and by foregoing “business as usual.”
The first step towards change is full recognition of the situation. In the case of Haiti, this means recognizing the marked failure of foreign recovery and development assistance to date. It is pointless to blame any particular institution or individual for this: The current state of Haiti is the culmination of generations of efforts and decisions, good and bad, combined with rapid population growth and an inherent vulnerability to natural hazards. (Editor’s note: according to the UN, Haiti’s fertility rate tripled in the immediate aftermath of the earthquake last year.)
The second step is planning. While relatively solid recovery plans have been developed by the government of Haiti with international assistance, their implementation has not so far met with success, due to four interlinked problems.
First, the humanitarian imperative for urgent and chronic relief is overrunning all good intentions for recovery and development – it is politically impossible, inhumane, and simply unwise to ignore the basic resource needs of a cholera epidemic and a million people living in tents.
Second, nothing suppresses development investments like political violence and uncertainty: Few donors, and even fewer companies, will invest while riots and political uncertainty paralyze the country and destroy its reputation.
Third, the planning process is necessarily democratic and participatory; as a result, however, virtually all of the country’s needs are listed with no reliable process of thematic or geographic prioritization.
Finally – and perhaps most importantly – although the plans are official and uncontested, they generally lack broad credibility and commitment. Weary aid workers, government officials, donors and the general public look back at the fate of previous plans and, not surprisingly, expect these latest efforts to fail just as others have before.
Regenerating Haiti
Unlike virtually all other aid organizations I have met in Haiti, the team behind the Haiti Regeneration Initiative (HRI) has fortunately been given the vital time and seed funding to reflect on these issues and try something really different. After two years of preparation, on January 4, 2010, we launched a long-term rural sustainable development initiative for the southwestern tip of Haiti. The Côte Sud Initiative aims to transform the lives and the degraded environment of 200,000 people living in one of the poorest yet most beautiful parts of Haiti.
This specific initiative will only directly assist two percent of the population of Haiti, but just as importantly, we aim to demonstrate that sustainable development is truly possible in this country. Because national-scale issues require national-scale efforts, we also aim to promote change through dialogue and assisting the government of Haiti to develop and deliver on sustainable development plans that work. This is the primary mission of the HRI.
We must arrest the long-term decline as soon as possible. This includes, but is not limited to, basic recovery from the earthquake. At the same time, we need to establish the foundations for the long-term radical changes that are an absolute prerequisite to achieving sustainable development in Haiti. We must prepare to turn the vicious circles into virtuous ones.
So what are the short- to medium-term priorities?
The first is political stabilization, as vital foreign aid and direct foreign investment will simply not arrive in the face of such negative news and uncertainty.
Second, a massive aid investment in potable water and sanitation is required to suppress cholera in the longer term. No country can develop in the midst of recurrent major epidemics. This investment needs to be designed for sustainability; in other words, infrastructure needs to be accompanied by realistic, locally financed mechanisms for maintenance. Otherwise it will become useless within weeks of installation.
Third, persistence is needed on the current debris clearance and rebuilding efforts; we know from many other countries that such efforts can take years to be completed.
Finally, development aid should move out of Port-au-Prince and into the regions. In 2010, the massive influx of earthquake relief and reconstruction aid actually increased the economic pull of the capital and exacerbated existing urban problems.
What to do to prepare for the long term? Implementing radical change requires political support and even cultural reform, so in addition to good ideas, the HRI partnership will work hard to develop a sense of national ownership of the solutions as well as the problems.
Many of the ideas are not new: mildly decentralized development, diversified and value-added agriculture, niche tourism, improved aid coordination, public-private partnerships, etc.
Many, however, are radical, including a proposed paradigm change on migration and remittances, education, food security and import policies, widespread privatization, harsh revisions and rebuttals of traditional development models and assumptions, and adaptation to the new types of religious NGOs. These are just a few of the concepts and opportunities we have identified and will work to make a reality in Haiti.
Over the next few years, the HRI hopes to foster an intelligent and useful dialogue on sustainable development in Haiti. We look forward to having all of those who are concerned about and interested in helping Haiti join us in the debate.
Andrew Morton is the Haiti Regeneration coordinator and a senior staff member at UNEP. For more information on the Haiti Regeneration Initiative please see www.haitiregeneration.org.
Sources: BBC, Haiti Regeneration Initiative, United Nations Development Programme.
Image Credit: “Rebuilding as a community,” courtesy of flickr user Save the Children.